General Information about Zebeta
In conclusion, Zebeta is a extremely effective and protected medicine for treating hypertension. It helps decrease blood pressure ranges and reduce the risk of heart attack, stroke, and different cardiovascular illnesses. It is a well-tolerated medication, with minimal unwanted effects, and can be utilized together with different antihypertensive medicine for higher blood stress management. However, it is important to take Zebeta as prescribed and to work carefully with a health care provider to watch blood stress levels and regulate the dosage if needed. With proper use and administration, Zebeta can significantly enhance the quality of life for individuals with hypertension.
High blood pressure, also referred to as hypertension, is a typical condition that impacts hundreds of thousands of individuals worldwide. It is a serious danger factor for cardiovascular illnesses similar to heart assault and stroke. Therefore, it is essential to effectively manage and management high blood pressure to scale back the risk of those life-threatening situations. One medicine that has been proven to be efficient in treating hypertension is Zebeta.
Zebeta is commonly utilized in mixture with other antihypertensive drugs to attain higher blood strain management. It works well with diuretics (water pills), calcium channel blockers, or angiotensin-converting enzyme (ACE) inhibitors. Combining these medications can have a synergistic effect, leading to higher blood strain administration. However, it is crucial to seek the advice of a physician before starting any new treatment or altering the dosage of current ones.
Aside from treating hypertension, Zebeta has also been found to have other beneficial results. It is used to prevent chest ache (angina) and to enhance survival after a coronary heart attack. It has additionally shown to be effective in treating heart failure, a condition the place the center is unable to pump enough blood to fulfill the body's needs. By slowing down the heart fee and reducing the workload of the center, Zebeta might help improve heart function and signs associated with these conditions.
Many people with high blood pressure haven't any symptoms and may only know their blood pressure levels by way of regular check-ups with their doctor. If left untreated, hypertension can result in critical health issues corresponding to heart disease, kidney disease, and stroke. Zebeta ought to be taken exactly as prescribed by a well being care provider, and regular monitoring of blood pressure is critical to make sure the treatment is working successfully.
Like any medication, Zebeta has a quantity of potential unwanted effects, although not everyone experiences them. Common unwanted effects embody headache, fatigue, dizziness, diarrhea, and nausea. These unwanted side effects are often mild and subside with continued use, but if they persist or turn into bothersome, it's important to inform a doctor. Rare but critical side effects embody issue breathing, chest ache, and irregular heartbeats. If any of those occur, seek instant medical attention.
Zebeta, additionally identified by its generic name bisoprolol, is a beta-blocker that works by blocking the action of sure chemical compounds in the body that can improve blood stress and coronary heart rate. This leads to a decrease in blood pressure, making it an effective remedy for hypertension. Zebeta is available as an oral tablet and is usually taken as quickly as a day with or with out food.
Careful examination for kyphosis and measurement of height are useful for detecting significant height loss (>5 cm) associated with osteoporotic vertebral compression fractures that may be asymptomatic blood pressure medication classes zebeta 5 mg buy overnight delivery. Breast tissue is generally discoid and has a firm edge that can be palpated and "flipped up" to distinguish it from adipose tissue. With this technique, gynecomastia can usually be distinguished from excessive breast adipose tissue, called pseudogynecomastia, which is often associated with generalized obesity. Gynecomastia is usually bilateral and relatively symmetric, but occasionally it is asymmetric and more prominent on one side. The diameter of palpable breast tissue is used as an objective measure of gynecomastia. Gynecomastia of recent onset is usually tender on palpation, and men usually complain of nipple irritation associated with rubbing against clothing. Examination of the testes and scrotum may be performed with the patient either lying on his back or standing, but the latter position is preferred because it relaxes the scrotum, making some abnormalities. In patients with retractile testes positioned high in the scrotum, it may be possible to palpate the testes only after placing the scrotum in warm water, after a warm bath, or by having the patient assume a squatting position. Glandular breast tissue feels like a rubbery disc of tissue that extends concentrically from under the nipple and subareolar area and is firmer than the surrounding adipose tissue. The size of gynecomastia is estimated by measurement of the diameter of palpable breast tissue. Care must be taken not to include the head of the epididymis when estimating testis size. In these instances, testicular ultrasound may be required to confirm the presence of the testis, estimate its size, and detect abnormalities. The testicular examination in men with classical Klinefelter syndrome is notable for very small (usually <3 mL), firm testes. Differential Diagnosis Because sexual dysfunction, gynecomastia, and infertility are often presenting complaints in adults with androgen deficiency, it is important to consider the differential diagnosis of these conditions and to be familiar with other common causes of these manifestations when evaluating men who present with these complaints. These components may occur in isolation, but specific disorders of sexual function commonly occur together because these processes are interrelated and because a specific cause. Men with androgen deficiency often present with sexual dysfunction, and it is important to consider the differential diagnosis of this complaint in the evaluation. Androgen deficiency often results in reduced libido or sexual desire (hypoactive sexual desire disorder); loss or reduction of spontaneous evening and morning or sexually stimulated erections (erectile dysfunction); and, if severe, reduced or absent ejaculation. In many men with androgen deficiency, erectile response to intense erotic stimuli (and, occasionally, spontaneous erections) may be preserved, suggesting that the androgen requirement for sexual function is variable. Men with severe androgen deficiency may present with reduced ejaculation, but these individuals usually also complain of hypoactive sexual desire disorder and erectile dysfunction. Hypoactive Sexual Desire Disorder and Erectile Dysfunction nuclei, and prefrontal cortex) and the temporal lobe. Stimuli from these areas are relayed to the medial preoptic area, which serves to integrate central inputs and sends impulses to the paraventricular nuclei; these, in turn, send projections to the thoracolumbar and sacral spinal cord centers that regulate penile erection. This neural pathway explains why brain disorders that cause hypoactive sexual desire disorder are usually accompanied by varying degrees of erectile dysfunction (see later discussion). Clinically, libido may be influenced by previous or recent sexual activity and by experiences, psychosocial background, overall state of general health, androgen sufficiency, and brain function. The neurotransmitter systems that regulate the physiology of normal libido are not precisely known. The use of pharmacologic agents with dopamine receptor antagonist activity is frequently associated with reduced libido and erectile dysfunction. Hypoactive sexual desire disorder is defined as persistent or recurrent deficiency or absence of desire for sexual activity resulting in marked personal distress, interpersonal difficulty, or both150,154,155 and is estimated to affect more than 15% of men. The causes of hypoactive sexual desire disorder are primarily disorders that affect normal brain function and are usually associated with erectile dysfunction, particularly with the loss of spontaneous evening or morning erections (Table 19. Erectile dysfunction is defined as the inability to achieve or maintain penile erection that is adequate for completion of satisfactory sexual intercourse or activity. It is estimated to affect fewer than 10% of men younger than 40 years of age but approximately 50% of men between 40 and 70 years of age, with 35% of men in the latter age group having moderate or complete erectile dysfunction. Hypoactive Sexual Desire Disorder and Erectile Dysfunction Due to Brain Disorders. Psychogenic disorders commonly cause Libido, the desire or drive for sexual activity, is generated by external visual, auditory, and tactile stimuli, as well as internal psychic stimuli acting on cortical and subcortical brain regions such as the limbic system (amygdala, hippocampus, anterior thalamic hypoactive sexual desire and erectile dysfunction. These disorders include stress or preoccupation associated with life circumstances or situations, illness, marital discord, or underlying maternal transference or gender identity issues; performance anxiety associated with fear of failure or preoccupation with the adequacy of erections during sexual intercourse; major depression or dysthymia (moderate or complete erectile dysfunction occurs in 60% to 90% of men with moderate to severe depression); and major psychiatric illness such as psychotic or personality disorders. Testosterone treatment of severe androgen deficiency in young men usually improves sexual desire, interest, and thoughts; attentiveness to erotic stimuli; and the frequency, duration, and rigidity of spontaneous evening and morning erections. Anecdotally, some men with androgen deficiency due to severe hyperprolactinemia who are treated with testosterone alone do not fully recover sexual function and may require additional therapy with dopamine receptor agonists, but this has not been demonstrated conclusively. Dopamine receptor agonists lower elevated prolactin concentrations and may also have direct affects in the brain to activate neuronal systems involved in stimulating libido and erections. Structural brain disease, such as infiltrative or destructive lesions of the temporal lobe or limbic system, Parkinson or other neurodegenerative brain disease, or vascular brain disorders such as stroke or vasculitis, may reduce libido and spontaneous erections. Androgen deficiency is commonly associated with reduction or loss of libido and spontaneous erections. In contrast, older men with less severe androgen deficiency may have sexual dysfunction that is also related to underlying depression, chronic systemic illness, or use of certain medications. Efferent parasympathetic nervous system stimulation from the sacral center travels via the nervi erigentes (pelvic splanchnic nerve) and the pelvic plexus and enters the penis via the cavernosal nerve. This stimulation causes relaxation of the smooth muscles that form sponge-like interconnected trabecular spaces within the corpora cavernosa of the penis and vasodilation of the cavernosal arterioles and vascular sinusoids. As a result, blood flow and pressure into the trabecular spaces within the corpora increase several fold and cause engorgement of the penis (tumescence). Expansion of the trabecular spaces against the thick fibrous sheath (tunica albuginea) surrounding the corpora compresses subtunical venules and impedes venous outflow, resulting in sustained penile tumescence.
Contrary to earlier studies hypertension with cardiac involvement purchase zebeta 5 mg with visa, it is now evident that the older woman who is not Chapter 30 Osteoporosis: Basic and Clinical Aspects 1285 as physically active, and is not taking estrogen, is at extremely high risk of bone loss and subsequent fractures. The pathogenesis of this process is multifactorial, although dietary calcium deficiency, leading to secondary hyperparathyroidism, certainly plays some role. The average calcium intake of women in their eighth and ninth decades of life is now estimated to be between 800 and 1000 mg/day. Unfortunately, in most elders, bone formation is not enhanced, although the reasons for this are not entirely clear. Furthermore, among elders with poor calcium intake who live in northern latitudes, seasonal changes in vitamin D levels, lowering levels below 20 ng/mL, might aggravate bone loss. Many older individuals already have established osteoporosis, so coincidental vitamin D deficiency due to poor intake, absent sunlight exposure, or impaired conversion of vitamin D to its active metabolite can result in osteomalacia and aggravate preexisting osteoporosis. Priemel and associates287 reported that more than 50% of elders who presented with a hip fracture were vitamin D deficient. Combining vitamin D deficiency with inadequate calcium intake enhances the likelihood of rapid bone loss in a very susceptible population. This would shift the remodeling balance toward preserving intravascular calcium concentrations while inhibiting new calcium incorporation into the skeletal matrix. Although most postmenopausal women and older men do not have a definable secondary cause, those who do can be treated more effectively. Secondary Osteoporosis the division of osteoporosis into primary and secondary forms is somewhat arbitrary. For example, patients with diseases that lead to hypogonadism early in life are considered to have secondary Glucocorticoid-Induced Bone Loss the most common cause of secondary osteoporosis is glucocorticoid-induced bone loss, which is often a result of pharmacologic doses of steroids used to treat inflammatory or autoimmune disorders. Generally, it is considered that glucocorticoids have a dosedependent effect on the skeleton such that longer duration and higher doses of steroids are most likely to cause bone loss and fractures. However, there clearly are subsets of individuals who are more or less sensitive to the skeletal effects of high doses of glucocorticoids. As a clinical rule, those individuals with a cushingoid appearance and fat redistribution phenotypes almost always have low bone mass and fractures. In 1932, Harvey Cushing recognized the syndrome of endogenous steroid excess, which included marked osteopenia and fractures. In addition to having direct effects on the osteoclast and osteoblast, glucocorticoids also induce secondary hypogonadism and hyperparathyroidism, impaired vitamin D metabolism, muscle atrophy, and hypercalciuria. All of these factors contribute to a rapid and sustained loss of bone during the first few months of steroid therapy. Because the number of organ transplants has increased exponentially over the past decade, the prevalence of post-transplantation osteoporosis has risen substantially. Steroid-induced osteoporosis is now considered the second most common cause of low bone mass in the general population and one of the most common causes of osteoporotic fractures. Although there is no true dose-dependent effect on bone resorption, it is thought that prednisone doses as low as 5 mg/day may increase fracture risk. Therapy for steroid-induced bone loss centers on treating the underlying disease and reducing the dose of glucocorticoids to the lowest possible regimen. Barring that, several interventions have been shown to retard bone loss and prevent fractures. Adequate calcium and vitamin D intake is critical for every patient receiving glucocorticoids. Regulatory approval for the prevention and treatment of glucocorticoid-induced osteoporosis has been consistent for the group of bisphosphonates, including alendronate, risedronate, and zoledronic acid. Some anecdotal data support the use of gonadal steroids in this condition, but clearly bisphosphonates are superior. Osteoporosis Associated With Diabetes Mellitus Diabetes mellitus includes a group of heterogeneous metabolic disorders that in common show hyperglycemia. The association between diabetes mellitus and osteoporosis underpins several relevant aspects. First, energy metabolism integrates the whole body; as such, severe disorders affecting energy metabolism do not spare any single system or tissue. Second, the endocrine regulation of bone and energy metabolism is not restricted to classical glands and neural regulation. Au contraire, there is an intricate mutual regulation between energy metabolism and mesenchymal tissues, including bone. Estimated 10-year cumulative fracture risk at age 75 years in women (A) and men (B), calculated using the Cox proportional hazards regression model baseline survival function raised to the power of the relative hazard for each combination of diabetes group and T-score. First of all, obesity, which is the central determinant for the emergence of insulin resistance and hyperglycemia, has a positive effect on bone mass. Leptin and adiponectin have complex effects on bone, and there are still no conclusive results about their ultimate effects on bone. Recent studies called attention for the clinical relevance of this parameter, such as the association of saturated lipids with fracture in diabetic individuals. The top figure exhibits differences in unsaturated fat between male and female (female > male). The intricate relationship between bone and energy metabolism aggregates issues concerning the potential repercussions of osteoporosis therapy on glucose metabolism, on one side, and the effects of diabetes management on bone mass and fracture occurrence, on the other. Osteoblasts express insulin receptor, and the experimental silencing of insulin receptor specifically in osteoblasts results in both decreased bone mass and impairment in glucose tolerance. The acidic environment created by osteoclasts to elicit bone resorption promotes osteocalcin decarboxylation.
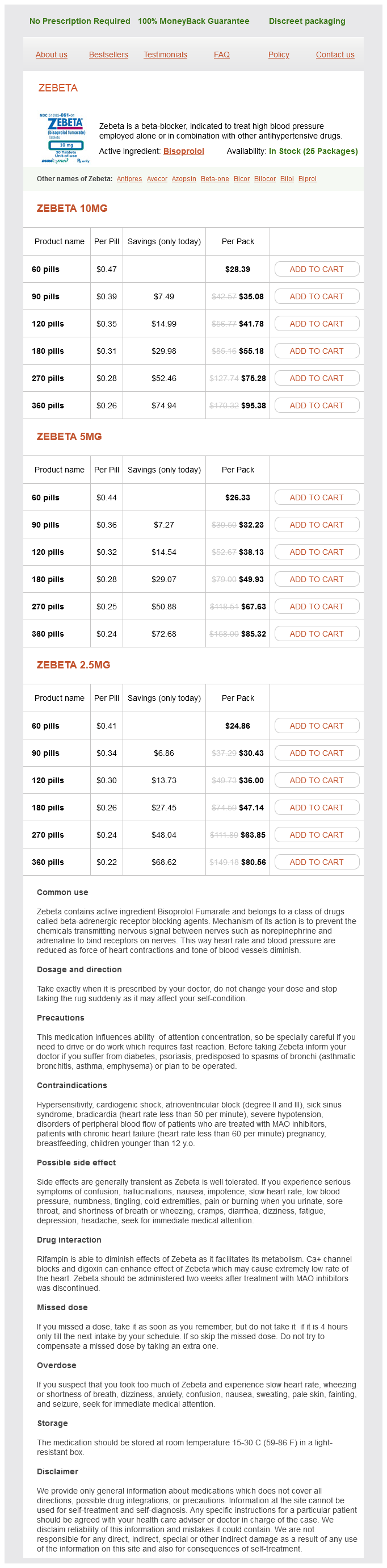
Zebeta Dosage and Price
Zebeta 10mg
- 60 pills - $28.39
- 90 pills - $35.08
- 120 pills - $41.78
- 180 pills - $55.18
- 270 pills - $75.28
- 360 pills - $95.38
Zebeta 5mg
- 60 pills - $26.33
- 90 pills - $32.23
- 120 pills - $38.13
- 180 pills - $49.93
- 270 pills - $67.63
- 360 pills - $85.32
Zebeta 2.5mg
- 60 pills - $24.86
- 90 pills - $30.43
- 120 pills - $36.00
- 180 pills - $47.14
- 270 pills - $63.85
- 360 pills - $80.56
Depending on the individual patient and his partners blood pressure medication good for kidneys order genuine zebeta on-line, this aroma might be pleasant or objectionable. Two additional transdermal formulations for the treatment of male hypogonadism have been approved in the United States. The advantages and disadvantages of these formulations are similar to those of AndroGel and Testim gels. There might be a higher risk of clinically important secondary transfer of testosterone to sexual partners with the use of Fortesta, and some men complain of dripping of the 2% Axiron testosterone solution from the axilla. In addition, some men might need to shave their axilla to apply Axiron; secondary transfer might be less likely to occur with axillary application, however. In one study, AndroGel contained testosterone amounts that were consistent and accurate; there was little variation within and between batches of AndroGel. However, in this same study, only 30% to 50% of batches of compounded testosterone formulations from 10 different pharmacies contained testosterone amounts within 20% of the stated dose; one compounded formulation had virtually no testosterone. This formulation is a small mucoadhesive tablet that contains 30 mg of testosterone in an oil-water emulsion carrier vehicle. The tablet contains polycarbophil, which, after application, remains attached to buccal mucosa until epithelial cells turn over (approximately every 1215 hours). The tablet is placed in the mouth between the inner cheek and gum, above the incisors, with the monoconvex side toward the gum and the flat side toward the cheek. After placement, the tablet softens and swells with hydration and becomes gelatinous and sticky, causing it to adhere to the gum. Testosterone is released at a controlled and sustained constant rate from the tablet through the buccal mucosa into the systemic circulation, circumventing first-pass hepatic metabolism. Striant tablets are placed on the buccal mucosa twice daily, with one tablet applied in the morning and removed after 12 hours and another applied in the evening on the opposite side. If the tablet falls off or is dislodged, a new tablet should be applied and left in place until the next regularly scheduled dose. The buccal tablet is removed by gently sliding it downward toward the incisor to avoid scratching the gum. Within-subject variation is shown by a shaded vertical line between the highest and lowest T concentration for each man. The dashed line denotes the reference range of serum T concentrations in adult men (3001000 ng/dL). Contact transfer of testosterone in saliva to others has not been reported to occur. In one study, approximately 10% to 15% of men developed gum or mouth irritation or inflammation, and 5% experienced an altered or bitter taste in the mouth. Initially, patients are aware and bothered by the tablet between their cheek and gum, resulting in premature discontinuation of the formulation. However, with continued use, the unusual sensation and awareness of the buccal tablet diminish and become less bothersome. Twice-daily application of Striant is required to sustain physiologic testosterone concentrations, and this makes compliance challenging. Informing patients that awareness of the buccal tablet diminishes over time and linking application of the transbuccal tablet to a routine daily activity such as morning and evening tooth brushing may help improve and maintain compliance. It is advised that there should be no nose blowing or sniffing for 1 hour after administration, and treatment should be discontinued temporarily during episodes of severe rhinitis. Although there is no interaction with symphathomimetic nasal decongestants, potential interaction with other intranasally administered medications is not known, so use with other nasal drugs is not recommended. When administered to hypogonadal men, mean serum testosterone concentrations peak in the high-normal range approximately 1 hour after administration and decline over 6 to 8 hours to concentrations at or slightly below normal. Testopel Pellets are recommended at doses that range from 150 to 450 mg testosterone. This minor surgical procedure is repeated three to four times yearly to maintain normal serum testosterone concentrations. Although spontaneous extrusion of pellets and local bleeding or infection may occur occasionally, these problems are uncommon in experienced hands. If adverse effects develop after implantation, a major concern is that removal of the testosterone pellets will be difficult, if not impossible. Therefore, the use of testosterone pellets is inappropriate for testosterone replacement in older patients who are predisposed to erythrocytosis and prostate disease during treatment. Testosterone Formulations Available Outside the United States Oral Testosterone Undecanoate. In many countries outside the United States, an oral 17-hydroxyl ester of testosterone, testosterone undecanoate (Andriol Testocaps, Organon, Oss, Netherlands), is available for testosterone replacement therapy in hypogonadal men. Serum testosterone concentrations peak approximately 5 hours after administration of testosterone undecanoate and fall to pretreatment concentrations within 8 to 12 hours. For testosterone replacement therapy, it is administered at relatively high doses, 40 to 80 mg two to three times daily (total dose, 80240 mg daily). Absorption of testosterone undecanoate requires concomitant food ingestion, and serum testosterone concentrations and clinical responses are highly variable. The use of castor oil and propylene glycol laurate instead of oleic acid, the vehicle used in the original formulation, permits storage at room temperature and extends the shelf life of Andriol Testocaps for up to 3 years while maintaining pharmacokinetic and pharmacodynamic characteristics similar to those of the original formulation. Testosterone concentrations fall quickly after discontinuation of testosterone undecanoate.