General Information about Xenical
Despite its advantages, Xenical just isn't a magic capsule for weight loss. It ought to be used in mixture with a wholesome and balanced food plan, regular exercise, and a dedication to long-term way of life adjustments. It is essential to note that Xenical could have some unwanted effects such as belly pain, flatulence, and oily stools. However, these may be managed by following a low-fat diet and are normally transient.
Apart from weight reduction, Xenical has additionally been discovered to be efficient in managing other health circumstances corresponding to high cholesterol and kind 2 diabetes. This is as a outcome of weight reduction can result in improved cardiovascular health and better management of blood sugar ranges.
The lively ingredient in Xenical is a particular and reversible inhibitor of gastrointestinal lipases. Lipases are enzymes produced by the pancreas and are liable for breaking down fats within the small intestine. Xenical works by forming a covalent bond with the active serine portion of the gastric and pancreatic lipases. This inhibits the enzyme's ability to break down food fat, stopping the absorption of triglycerides, free fatty acids, and monoglycerides.
Xenical, also referred to as Orlistat, is a medication that is generally used for weight reduction. It works by inhibiting the enzymes liable for breaking down fat in the digestive system. This leads to a lower within the absorption of calories from meals, resulting in weight loss.
The action of Xenical can be specific, that means it only inhibits lipases and does not have an effect on different enzymes or processes within the body. This makes it a highly effective drug for weight reduction, with minimal unwanted effects. In addition, Xenical is reversible, that means its effects are temporary and can be reversed as quickly as the drug is discontinued.
One of the most important benefits of Xenical is that its therapeutic impact is carried out in the lumen of the stomach and small gut. This signifies that the drug doesn't enter the systemic circulation and its action is restricted to the world where it is wanted. This makes it a safer and extra targeted possibility for weight reduction compared to other medicines that will have a systemic impact.
Clinical research have proven that Xenical can outcome in a significant discount in weight, especially when mixed with exercise and a nutritious diet. In reality, studies have shown that sufferers who took Xenical for one year lost an average of 10% of their initial body weight. This is a major decrease and might have a constructive impression on total well being and well-being.
In conclusion, Xenical is a robust and effective treatment for weight loss. Its specific and reversible action in the digestive system makes it a protected and focused option for those looking to lose weight. However, it may be very important seek the assistance of with a physician earlier than starting any weight loss medication and to make way of life modifications for long-term success.
Urinary neutrophil gelatinaseassociated lipocalin as a marker of acute kidney injury after orthotopic liver transplantation weight loss using phentermine order cheap xenical. Prophylactic fenoldopam for renal protection in sepsis: a randomized, double-blind, placebo controlled pilot trial. Beneficial impact of fenoldopam in critically ill patients with or at risk for acute renal failure: a meta-analysis of randomized clinical trials. The Society of Thoracic Surgeons: 30-day operative mortality and morbidity risk models. Acute kidney injury following cardiac surgery: current understanding and future directions. The body and cardiovascular system are exposed to many challenges, such as neurohumoral adaptations, evaporation, fluid redistribution, and blood loss, that necessitate interventions. To achieve this, fluids are administered intravenously following protocols based on tradition, expert recommendations, and often limited evidence. There is an ongoing debate concerning the ideal composition and amount of intravenous fluids necessary for perioperative management. There are a few simple tests or physical maneuvers that can assess reliably either the level of hydration or the intravascular volume status. The clinician usually must rely on indirect nonspecific clinical signs to estimate the volume status of the cardiovascular system. Very few healthy stable surgical patients admitted for elective minor operations require significant amounts of fluid, and thus the perioperative fluid management of these patients is straightforward. It carefully describes physiological principles about fluid shifting in the body and responses to fluid challenges. It further describes different monitoring principles on how to estimate fluid volumes. Water constitutes about 60% of body weight and is unequally distributed between extracellular and intracellular spaces. However, evidence suggests that several currently used monitors have limitations in measuring the adequacy of intravascular volume. However, this static concept hardly reflects the complexity of how fluids dynamically distribute over time. The interstitial fluid volume contains water but is mainly bound by a gel-like composition of proteoglycan filaments and collagen fibers. The predominant intracellular cation K+ (potassium ion) has an intracellular concentration of approximately 150 mM. The volume of erythrocytes can be determined by isotope labeling with chromium 51 (51Cr) and technetium 99 (99Tc), for example, but there are other nonradioactive methods such as labeling erythrocytes with fluorescein. Anthropometric predictions of various physiologic properties depend on height, weight, age, gender, and race; these population models naturally result in various degrees of inaccuracy when applied to individuals. Water intake includes ingested liquids plus an average of 750 mL ingested in solid food and 350 mL generated metabolically. Renal water handling has three important components: (1) delivery of tubular fluid to the diluting segments of the nephron, (2) separation of solute and water in the diluting segment, and (3) variable reabsorption of water in the collecting ducts. This concentrated fluid is then diluted by active reabsorption of electrolytes in the ascending limb of the loop of Henle and distal tubule, both of which are relatively impermeable to water. As fluid exits the distal tubule and enters the collecting duct, osmolality is ~50 mOsm/ kg. Vasopressin binds to V2 receptors along the basolateral membrane of the collecting duct cells and stimulates synthesis and insertion of aquaporin-2 water channels into the luminal membrane of collecting duct cells to facilitate water permeability. Daily requirements for Na+ and K+ are approximately 75 mEq/ day and 40 mEq/day, respectively, although wider ranges of Na+ intake than K+ intake are physiologically tolerated because conservation and excretion of Na+ are more efficient than of K+. Therefore healthy 70-kg adults require 2500 mL/day of water containing a Na+ of 30 mM and a K+ of 15 to 20 mM. The main nonfluid components are fibrils and the interstitial ground substance that can be subdivided into a colloid-rich and a water-rich phase. The amorphous ground substance or gel-like matrix is produced by the same cell types as the fibrillar components. Plasma proteins passing the capillary wall are mainly restricted to a random network of interstitial channels corresponding to colloid-poor, water-rich areas. The physiologic distribution is maintained by biologic barriers and adenosine triphosphaterequiring pumps. The vascular wall is impermeable to larger molecules or proteins, with normal fluid distribution subject to an intact inner lining of the endothelial wall (glycocalyx). However, deterioration of the glycocalyx, as seen in systemic inflammatory conditions, is of greater importance than interstitial protein concentration for fluid escape through the endothelial barrier. These are mainly syndecans and membrane-bound glypicans that contain heparan sulfate and chondroitin sulfate chains. Together with some plasma proteins that are membrane bound, hyaluronan, and dissolved glycosaminoglycans, the inner endothelial surface layer is tens of nanometers thick. Water intake is required to offset gastrointestinal, urinary and insensible losses. In this pathway, decreased stretch in the baroreceptors of the aortic arch and carotid body and stretch receptors in the great veins, pulmonary vasculature, and atria result in increased sympathetic tone. Increased sympathetic tone, in combination with decreased renal perfusion, leads to renin release and formation of angiotensin I from angiotensinogen. Abbreviations refer to the Starling formula, which is modified by the existence of the glycocalyx.
This has been met with some controversy given the questionable scientific foundation weight loss 4 doctors select nutraceuticals xenical 120 mg generic, the pharmacologic heterogeneity of the cannabis in terms of its numerous active compounds, and the awkward political reality that cannabis continues to be seen as an illicit substance in the eyes of the Drug Enforcement Agency. Considering these developments it is no surprise that the use of cannabis for treatment of symptoms common to many disease states continues to dominate political debates both in the United States and worldwide. In January 2017 the National Academies of Sciences, Engineering, and Medicine released a comprehensive review of research on the health effects of cannabis use. Among the nearly 100 conclusions made by the expert ad hoc committee was the following statement with regards to use of cannabis in the treatment of chronic pain: "There is substantial evidence that cannabis is an effective treatment for chronic pain in adults. Furthermore, the long-term, systemic effects of chronic cannabis use remain largely unknown. Pregabalin is approved for partial seizures, painful diabetic peripheral neuropathy, postherpetic neuralgia, and fibromyalgia. This article presents an extensive head-to-head comparison of the pharmacokinetics of pregabalin and gabapentin while highlighting their differences in bioavailability and the rationale behind maximal dose titration. Does multimodal analgesia with acetaminophen, nonsteroidal antiinflammatory drugs, or selective cyclooxygenase-2 inhibitors and patient-controlled analgesia morphine offer advantages over morphine alone This is an important work that carefully analyzes the effects of nonopioid analgesics on various perioperative outcomes. Their data confirmed the safety concerns of rofecoxib but supported the relative cardiovascular safety of celecoxib and naproxen, and raised concerns about the safety of diclofenac. Plasma levels and tricyclic antidepressant therapy: part 2 Pharmacokinetic, clinical and toxicologic aspects. This confirmed a modest utility for chronic neuropathic pain, but showed a lack of efficacy for acute pain. This is a very nice overview of the physiology of prostanoids and how nonsteroidal antiinflammatory agents modulate their function. Analgesics for pain after traumatic or orthopedic surgery: what is the evidence-a systematic review. Comparing analgesic efficacy of non-steroidal anti-inflammatory drugs given by different routes in acute and chronic pain: a qualitative systematic review. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis Effects of nonsteroidal antiinflammatory drugs on platelet function and systemic hemostasis. Cyclooxygenase-2 selective nonsteroidal antiinflammatory drugs and the risk of ischemic stroke: a nested case-control study. Efficacy and safety of the cyclooxygenase 2 inhibitors parecoxib and valdecoxib in patients undergoing coronary artery bypass surgery. Cardiovascular safety of the cyclooxygenase-2 selective inhibitors parecoxib and valdecoxib in the postoperative setting: an analysis of integrated data. Cardiovascular risk and inhibition of cyclooxygenase: a systematic review of the observational studies of selective and nonselective inhibitors of cyclooxygenase 2. Indomethacin and aspirin: effect of nonsteroidal anti-inflammatory agents on the rate of fracture repair in the rat. Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. The effect of postoperative nonsteroidal antiinflammatory drug administration on spinal fusion. Ketorolac and spinal fusion: Does the perioperative use of ketorolac really inhibit spinal fusion High-dose ketorolac affects adult spinal fusion: a meta-analysis of the effect of perioperative nonsteroidal anti-inflammatory drugs on spinal fusion. Clinical patterns of hypersensitivity to nonsteroidal anti-inflammatory drugs and their pathogenesis. Effects of hypotensive anesthesia, nonsteroidal antiinflammatory drugs, and polymethylmethacrylate on bleeding in total hip arthroplasty patients. Non-steroidal anti-inflammatory drugs and perioperative bleeding in paediatric tonsillectomy. Pathophysiologic factors affecting the pharmacokinetics of nonsteroidal antiinflammatory drugs. Comparison of morphine, ketorolac, and their combination for postoperative pain: results from a large, randomized, double-blind trial. Cannabinoid receptor-mediated antinociception with acetaminophen drug combinations in rats with neuropathic spinal cord injury pain. Acetaminophen-induced nephrotoxicity: pathophysiology, clinical manifestations, and management. Intravenous paracetamol as adjunctive treatment for postoperative pain after cardiac surgery: a double blind randomized controlled trial. Efficacy and safety of single and repeated administration of 1 gram intravenous acetaminophen injection (paracetamol) for pain management after major orthopedic surgery. Upregulation of prostaglandin E2 and interleukins in the central nervous system and peripheral tissue during and after surgery in humans. Effects of perioperative administration of a selective cyclooxygenase 2 inhibitor on pain management and recovery of function after knee replacement: a randomized controlled trial. Combination therapy for pain management in inflammatory arthritis (rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, other spondyloarthritis). Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review.
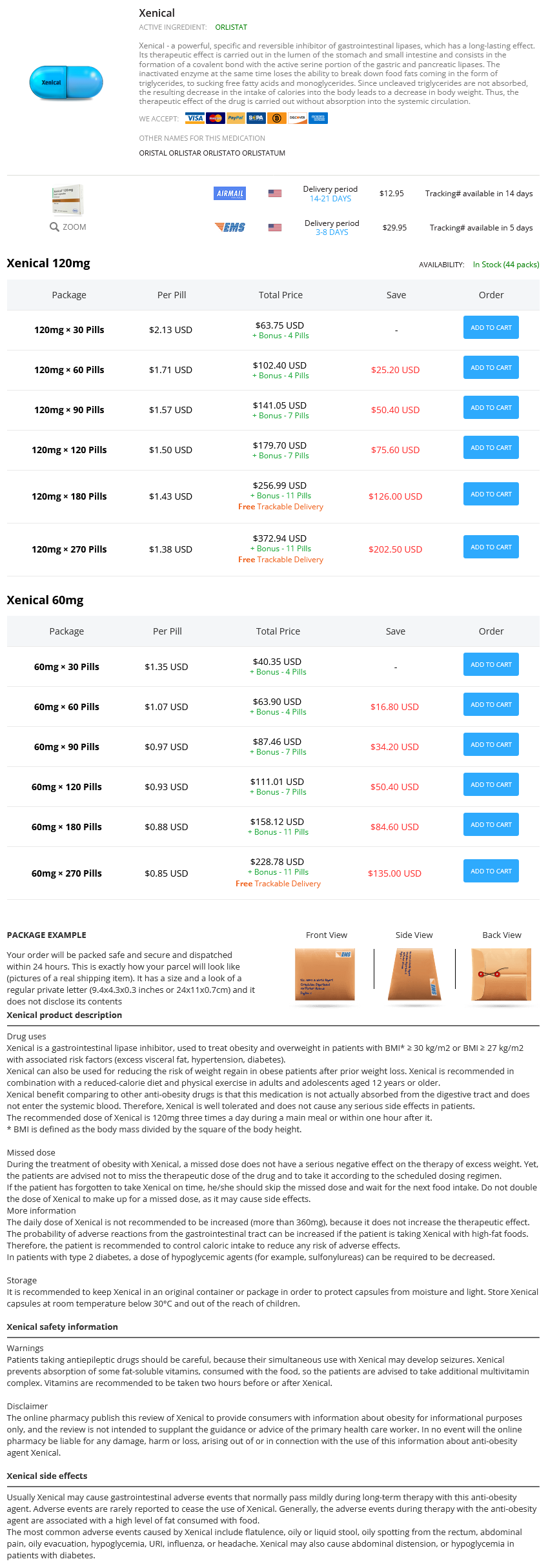
Xenical Dosage and Price
Xenical 120mg
- 30 pills - $63.75
- 60 pills - $102.40
- 90 pills - $141.05
- 120 pills - $179.70
- 180 pills - $256.99
- 270 pills - $372.94
Xenical 60mg
- 30 pills - $40.35
- 60 pills - $63.90
- 90 pills - $87.46
- 120 pills - $111.01
- 180 pills - $158.12
- 270 pills - $228.78
Untoward hypertension can occur following its use to treat regional anesthetic-induced hypotension because sympathetic tone returns as the spinal anesthetic recovers before the action of methoxamine dissipates weight loss meals order genuine xenical line. Midodrine Midodrine is an orally absorbed 1 agonist with a half-life of about 3 hours and duration of action of 4 to 6 hours. It is used to treat dialysis-related hypotension or autonomic failure resulting in postural hypotension, but hypertension is a possible effect when patients are supine. It is likely that some of the effects from 2-receptor agonists are from actions at nonadrenergic imidazoline receptors. The 2 receptor mediates sedation and hypnosis, sympatholysis, neuroprotection, diuresis, and inhibition of insulin and growth hormone secretion. The locus coeruleus is an important modulator of wakefulness and the major site of the sedative/hypnotic actions of the 2 agonists. It is available in 100-, 250-, and 300-µg tablets for oral administration, a transdermal patch releasing 150 to 200 µg over 24 hours, and an injectable solution of 150 µg/mL. Clonidine should not be withheld before surgery because acute withdrawal can result in rebound hypertension. When given in this manner, bradycardia and sedation can occur but respiratory drive is maintained. Sedation is described as "arousable sedation" much like natural sleep, consistent with effects on central sleep mechanisms. Hypotension and bradycardia are common side effects, and bradyarrhythmias and sinus arrest are rare but potential serious adverse events. These agents work by reducing bronchial airway resistance via smooth muscle relaxation. Metaproterenol (orciprenaline), albuterol, salmeterol, and isoetharine (isoetarine) are inhaled, thereby reducing their systemic side effects. These reach therapeutic concentrations in the bronchi with minimal activation of cardiac and peripheral 2 receptors. In addition to bronchodilation, therapeutic effects include suppression of release of leukotrienes and histamine from mast cells and decreased microvascular permeability. However, at higher concentrations all currently used 2-selective agonists also stimulate 1 receptors, which increases the risk for arrhythmias (predominantly atrial fibrillation). Other potential adverse effects, particularly when given orally or parenterally, are skeletal muscle tremor, tachycardia, mismatching of pulmonary ventilation and perfusion, and pulmonary edema. Long-term use can lead to tolerance, bronchial hyperreactivity, and hyperglycemia in diabetic patients. Isoproterenol produces positive chronotropic and inotropic cardiac effects via 1-adrenoceptor stimulation, and bronchodilation and vasodilatation in vascular smooth muscle through 2 activation. The emergence of phosphodiesterase inhibitors to improve myocardial performance has also reduced the need for isoproterenol as an inotropic agent. Isoproterenol has been used to manage heart failure secondary to bradycardia, cor pulmonale, pulmonary hypertension, as a chemical "pacer" in third-degree heart block, and in torsades de pointes ventricular tachycardia. Dobutamine Dobutamine is a synthetic catecholamine obtained by substitution of a bulky aromatic group on the side chain of dopamine. The (-) isomer acts on 1-adrenergic receptors and increases vascular resistance, and the (+) isomer is a potent 1-adrenergic receptor agonist and a potent 1-adrenergic receptor antagonist that blocks the effects of (-) dobutamine (see Table 14. Thus it often improves cardiac output without major adverse effects on the myocardial oxygen supply/demand ratio because afterload is maintained, thereby improving coronary blood flow. Dobutamine is prepared in 5% dextrose in water because it is inactivated in alkaline solutions. Dobutamine is often used for nonexercise cardiac stress testing and for the treatment of acute heart failure, especially in patients being weaned from cardiopulmonary bypass. Terbutaline and Ritodrine Terbutaline can be administered orally, subcutaneously, or by inhalation. Terbutaline is used primarily long term for obstructive pulmonary disease, and acutely for status asthmaticus, bronchospasm, and acute anaphylactic shock, where it does not have the cardiac stimulating effects of epinephrine. Terbutaline and ritodrine are also tocolytic drugs used to manage premature labor contractions through relaxation of the myometrium via their 2 effect. Ritodrine is usually started intravenously and is continued orally if tocolysis is achieved. It is metabolized in the liver to inactive conjugates, and about half the drug is excreted unchanged in the urine. The mechanism of hypokalemia involves an insulin-mediated increase in uptake of extracellular K+ and/or increased sodium-potassium adenosine triphosphatase activity. Ephedrine is a natural product of the ephedra plant (Ephedra sinica), and is a mixed-acting, noncatecholamine sympathomimetic with both direct and indirect stimulating effects on - and -adrenergic receptors. It acts indirectly by competing with norepinephrine for local reuptake into synaptic vesicles, resulting in elevated concentrations of norepinephrine at receptor sites. Intravenous effects resemble those of epinephrine, albeit with a less potent but longer-lasting effect. This is due to an effect of ephedrine to cause venoconstriction, thereby improving preload, cardiac output, and uterine blood flow. Ergot Alkaloids Poisoning caused by the fungus Claviceps purpurea on wheat or rye in the Middle Ages was associated with mental disturbances and severe, painful peripheral vasoconstriction frequently leading to gangrene of the extremities. Contraction of vascular smooth muscle leads to coronary, cerebral, and peripheral vasoconstriction.