General Information about Vantin
Vantin is usually taken twice a day, with or without food. The dosage and duration of treatment will range depending on the type and severity of the an infection, as well as a person's age and medical history. It's essential to observe the prescribed therapy plan and complete the full course of antibiotics, even if signs improve. Stopping medication too early can result in the micro organism not being totally eradicated, leading to a recurrence of the an infection.
Like any medication, Vantin might cause side effects in some individuals. Common unwanted effects may embrace nausea, diarrhea, upset stomach, and headache. If these symptoms persist or turn into severe, it is important to contact a physician. Additionally, as with all antibiotic, there's a risk of growing an allergic response. Seek quick medical attention if any signs of an allergic response happen, corresponding to rash, itching, swelling of the face or throat, or issue respiration.
Vantin works by preventing the expansion and copy of bacteria in the physique. It does this by interfering with the production of the bacterial cell wall, which is essential for the bacteria’s survival. Without a cell wall, the micro organism are unable to maintain their form and eventually die off. This helps to stop the spread of infection and permits the body's immune system to battle off the remaining bacteria.
Vantin is an oral antibiotic, obtainable in tablet kind or as a suspension. It is usually used to deal with infections of the respiratory tract, together with pneumonia, bronchitis, and sinusitis. It may additionally be used to treat skin and delicate tissue infections, in addition to certain forms of urinary tract infections. Vantin can also be efficient in treating some sexually transmitted infections, such as gonorrhea.
It is important to tell your physician of some other medicines you take, together with over-the-counter medicines and supplements, as they might work together with Vantin. In specific, it could be very important keep away from taking Vantin with antacids or iron dietary supplements, as they'll lower the effectiveness of the antibiotic.
Vantin, also known by its generic name cefpodoxime, is a generally prescribed antibiotic used to treat a wide selection of bacterial infections. It belongs to the class of antibiotics called cephalosporins, and is often prescribed for the therapy of gentle to moderate infections. Let's take a better look at what Vantin is, the method it works, and what situations it can effectively treat.
In conclusion, Vantin is a extremely efficient and commonly prescribed antibiotic for the remedy of mild to moderate bacterial infections. It is necessary to observe the prescribed treatment plan and to take the full course of medicine in order to guarantee complete eradication of the infection. If you expertise any unwanted effects or have any considerations, it may be very important consult your doctor. With proper use, Vantin can help alleviate symptoms and help in a swift restoration from bacterial infections.
It's necessary to note that Vantin is not effective against all forms of bacteria. It particularly targets certain types of bacteria, together with Streptococci, Staphylococci, and a few strains of E. coli. Therefore, it is necessary to solely take Vantin for infections which may be attributable to these bacteria, as utilizing it for different forms of infections can contribute to the development of antibiotic resistance.
Hysteroscopic sterilization has advantages of avoiding abdominal incisions and can be performed under local anaesthesia or simple analgesia in an outpatient setting antimicrobial products for mold cheap vantin 100 mg buy online. It is particularly suitable for women who present an anaesthetic or operative risk. The Essure system uses microinserts that are expanding springs (2 mm diameter and 4 cm in length) made of titanium, stainless steel and nickelcontaining Dacron fibres. A microinsert is placed in the proximal section of the fallopian tube under hysteroscopy. The success of the procedure is verified by the absence of sperm on semen analysis (and contraception must be continued until this time). The time to azoospermia depends on the frequency of intercourse, but it is estimated that 20 ejaculations are required. Reversal of vasectomy is associated with patency rates of almost 90% in some series. Pregnancy rates are much less (up to 60%), possibly due to the development of antisperm antibodies. Barrier methods Male and female condoms the male latex condom is cheap, widely available over the counter and, with the exception of the occasional allergic reaction, is free from side effects. The female condom is a polyurethane sheath (single size) with flexible polyurethane ring and is placed inside the vagina. Diaphragm and cervical cap the diaphragm and cap are less popular than male condoms. In order to select the correct size of diaphragm, a vaginal examination is conducted. Latex allergy, recurrent local vaginal infections and recurrent urinary tract infection are possible side effects. Complications Scrotal bruising occurs in almost everyone, and haematoma (12%) and wound infection (up to 5%) are common minor complications. The development of antisperm antibodies (thought to be in response to leakage of sperm) occurs in most men and appears to be harmless unless restoration of fertility is desired. Small inflammatory granulomas can form at the ends of the vas but can be effectively excised. Chronic postvasectomy pain (testicular, scrotal, pelvic or lower abdominal) is a persistent pain of unknown cause. Concerns have been raised linking vasectomy with an increased risk of atherosclerosis, testicular cancer, prostatic cancer and other, mainly autoimmune, diseases. Several large studies have failed to substantiate these concerns and there seems to be no biological plausibility for such a link. Assessment and counselling for sterilization Couples sterilized at a young age, immediately after delivery or at the time of an induced abortion are more likely to experience regret. A history should be taken and scrotal or bimanual pelvic examination should be carried out either at initial consultation or before commencing the procedure. Reversal of sterilization Reversal of female sterilization (tubal reanastomosis) involves laparotomy, does not always work (microsurgical techniques have around 70% success) and carries a significant risk of ectopic pregnancy (up to 5%). Reversal of sterilization with microinserts cannot be achieved via fallopian tube reanastomosis, and therefore consideration should All barrier methods have high failure rates when used typically. For calendar or rhythm method, the woman calculates the fertile period according to the length of her normal menstrual cycle. The first day of the fertile period is calculated as the length of the shortest cycle minus 20 days, and the last day of the fertile period as the longest cycle minus 10 days. Therefore if cycle length varies from 25 to 30 days, the potential fertile period and days when intercourse should be avoided are days 520. Contraception and Sterilization 951 the mucus or Billings method relies on identifying changes in the quantity and quality of cervical and vaginal mucus. As circulating oestrogens increase with follicle growth, the mucus becomes clear and stretchy allowing the passage of sperm. With ovulation, and in the presence of progesterone, mucus becomes opaque, sticky and much less stretchy. Intercourse must stop when fertiletype mucus is identified and can start again when infertiletype mucus is recognized. Progesterone secretion is associated with a rise in basal body temperature of about 0. Other signs/symptoms, such as ovulation pain, position of cervix and dilatation of the cervical os, can be used to help define the fertile period. Persona may be used by women to detect the fertile phase of the cycle); the monitor displays a green light for the nonfertile phase and a red light for the fertile phase. An increasing number of fertility apps for mobile phones, where the user inputs cycle length and/or symptoms such as basal body temperature, are being adapted for contraceptive purposes. Whatever method is used, many couples find it difficult to abstain from intercourse during the fertile period. It reduces the pain of endometriosis and adenomyosis and protects against unopposed oestrogen. Lactational amenorrhoea method Breastfeeding delays the resumption of fertility after childbirth and the length of the delay is related to the frequency and duration of breastfeeding episodes. A woman who is fully or nearly fully breastfeeding and who remains amenorrhoeic has less than a 2% chance of pregnancy during the first 6 months after childbirth (lactational amenorrhoea method). Contraception can be started at any time if it is reasonably certain that a woman is not already pregnant. Immediately after pregnancy is a key time to provide contraception, since fertility and sexual intercourse resume quickly.
In general antibiotics to treat sinus infection best 100 mg vantin, before insertion of the device or anastomosis of an iliac conduit, systemic heparin is administered. This access is used for the insertion of a pigtail arteriography catheter over a guidewire. Arteriography of the aortic arch, descending and proximal abdominal aorta is performed to mark and roadmap the location of the arch and mesenteric vessels. Adequate imaging and arteriography of the aorta require rapid injection of contrast using a power injector. The access to the aorta for the insertion of the device is obtained using an exchange length guidewire under fluoroscopic control. A utility catheter (Glide catheter) is inserted over the guidewire to maintain access. The large sheath with the tapered dilator is inserted over a stiff guidewire (Lunderquist or Amplatz super stiff guidewire). All guidewire, catheter, and sheath insertions must be performed under fluoroscopic control to avoid false passages and intimal injury. Under fluoroscopic control, the device is inserted over the stiff guidewire and deployed. Endografts of the same diameter or one to two sizes larger can be deployed overlapping a previously inserted graft. Sizing of Additional Endografts Inadvertent insertion of a smaller endograft inside a larger graft will result in lack of fixation and migration of the smaller graft. Excessive oversizing of an endograft inside a smaller graft may result in crimping and occlusion of the larger graft. Inadequate Proximal Neck If a normal segment of the aorta 23 to 37 mm in diameter of at least 2 cm in length is not present distal to the left subclavian artery, then deployment in the arch between the left common carotid and left subclavian arteries may be considered. Occlusion of Subclavian Artery In general, occlusion of the left subclavian artery with the endovascular graft may be well tolerated without adjunctive procedures. These include patients with a diminutive right vertebral artery and a dominant left vertebral artery who would be at risk for a posterior cerebral vascular accident. Patients who have previously undergone coronary artery bypass grafting of the left anterior descending coronary artery using the left internal thoracic artery also require a patent left subclavian artery. In these patients, a left carotid-subclavian bypass must be performed before endografting of the descending thoracic aorta to avoid cerebral or cardiac complications. The left carotidsubclavian bypass may be performed through a small supraclavicular exposure of the left carotid and subclavian arteries. Inadequate Distal Cuff In some patients, the distal aneurysm extension is close to the celiac artery such that a 2 cm length of the aorta proximal to the celiac axis in not present. The thoracoabdominal repair should be considered for most patients with low risk for open surgery. In higher risk patients, de-branching of the abdominal aorta may provide adequate length for endovascular repair. In this combined open-endovascular approach, the celiac and superior mesenteric arteries may be bypassed using grafts from the terminal aorta or the iliac arteries. These patients still require a transperitoneal abdominal or retroperitoneal approach to the abdominal aorta. After rerouting of the mesenteric vessels, the thoracic portion of the aorta can be repaired using an endograft. Patients at High Risk for Spinal Ischemia Some patients may have previously undergone repair of abdominal aortic aneurysms or may have occlusion of the internal iliac arteries. Other patients may have extensive aneurysms from the proximal arch to the level of the diaphragm requiring multiple overlapping endografts. These patients have been found to be at increased risk for spinal cord ischemia after endovascular repair of thoracic aortic aneurysms. Occlusion of the left subclavian artery with the endovascular graft may exacerbate this risk due to compromise of the vertebral artery as a collateral to the anterior spinal artery. In these patients, insertion of a lumbar drain preoperatively may reduce the risk. In addition to the lumbar drain, avoiding intraoperative and postoperative hypotension is an important consideration to maintain spinal perfusion. Endoleaks Some aneurysms maintain continuity with the circulation after placement of endovascular grafts. These endoleaks may be recognized at the time of treatment on the completion angiogram of the aorta. Frequently, the endoleaks are recognized on follow-up imaging such as computed tomography with contrast. Depending on the type and location of the endoleaks, various therapeutic options may be available. Type I leak is the most commonly encountered type, and involves a leak from the proximal or distal fixation site. These should be treated routinely, usually with additional endografts within the old graft. If persistent, treatment involves the insertion of a covered stent-graft (endograft) inside the original graft. Type V or endotension refers to the expansion of the aneurysm despite treatment without any documented leak into the aneurysm sac, potentially through the graft fabric. The patients who have undergone endovascular repair of thoracic aortic aneurysms are followed up closely with serial computed tomography of the chest, abdomen, and pelvis. Routinely, after an uneventful repair, the first postoperative scan is obtained 2 to 4 weeks after surgery and annually thereafter. A: the distal ends of graft limbs are anastomosed to the left subclavian, the common carotid, and the innominate arteries. In this combined open-endovascular procedure, the innominate, left carotid and left subclavian arteries are bypassed using a graft(s) from the ascending aorta.
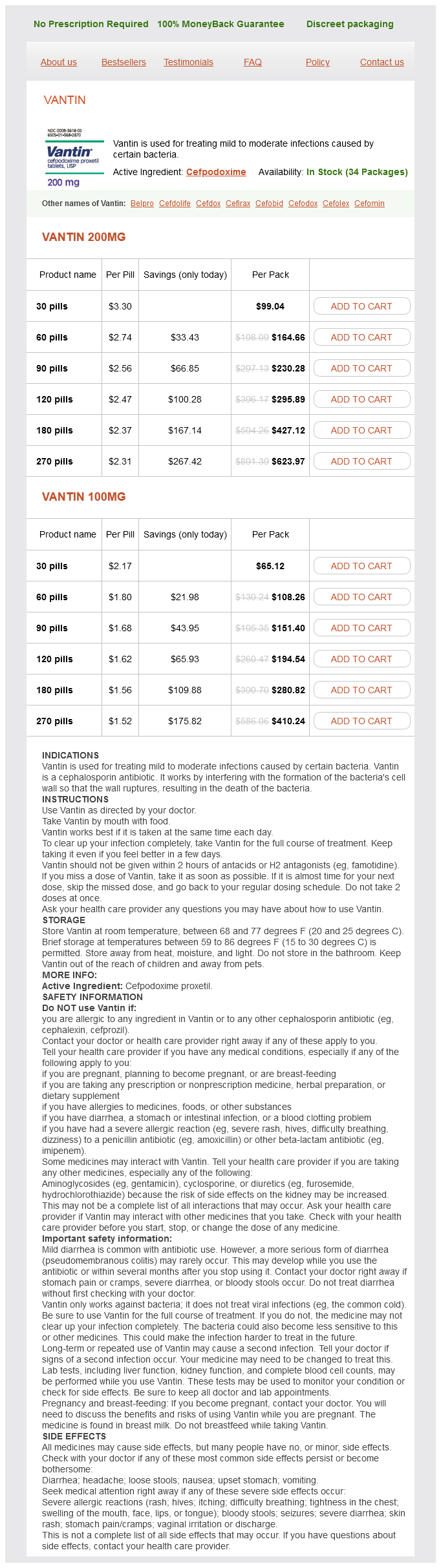
Vantin Dosage and Price
Vantin 200mg
- 30 pills - $99.04
- 60 pills - $164.66
- 90 pills - $230.28
- 120 pills - $295.89
- 180 pills - $427.12
- 270 pills - $623.97
Vantin 100mg
- 30 pills - $65.12
- 60 pills - $108.26
- 90 pills - $151.40
- 120 pills - $194.54
- 180 pills - $280.82
- 270 pills - $410.24
These latter results should be interpreted carefully because the procedure frequently disturbs the infant and alters blood gases infection of the cervix buy vantin 200 mg low cost. An alternative is to obtain blood samples from the peripheral capillary bed of the medial or lateral plantar surface. These are obtained after warming of the area, which produces hyperemia or "arterialization. Because blood cell metabolism continues, reducing the time from sampling to analysis and cold temperature storage and transport attenuate its effects. During conditions such as transport or when the turnaround time is important, bedside portable blood analysis devices have proven to be most effective (Murthy et al, 1997). During measurement of TcPo2, oxygen diffusing from the capillaries to the skin is reduced by the electrode, and the resulting electrical current is proportional to the Po2 of the capillary bed. For this reason, accuracy of TcPo2 depends on electrode temperature with improved accuracy at or above 43° C (Huch et al, 1976). However, conditions such as arterial hypotension and acidosis often result in underestimation due to insufficient skin perfusion (Versmold et al, 1979). This changes the electric potential between a reference and the electrode that is then translated into TcPco2. TcPco2 measurements can also be affected by conditions affecting peripheral perfusion (Peabody and Emery, 1985) and tend to overestimate Paco2 in hypercapnia as local perfusion decreases (Martin et al, 1988). TcPco2 measurements have also been shown to be tightly correlated to capillary Pco2. Although capillary blood gases may not be the optimal reference, these are often the only available method for long-term monitoring because indwelling lines are available only during the acute phase of respiratory failure. In preterm infants, TcPco2 may reduce the need for blood sampling and the number of painful punctures, but the main benefit is the ability to monitor continuously. For this reason, TcPco2 is commonly used as an adjunct to standard blood gas sampling to provide information on trends and respiratory stability. This is particularly useful in the management of invasive ventilatory support where close tracking of the effects of ventilator changes is required. Measurements of TcPo2 and TcPco2 require a period of stabilization after sensor application until skin perfusion increases. Similar to blood gas sampling, an air bubble transiently lowers TcPco2 and shifts TcPo2 toward the partial pressure of O2 in room air until the O2 is reduced. Transcutaneous measurements have an intrinsic delay with respect to changes occurring in the arterial blood. PetCo2 is obtained by infrared sensors placed mainstream or by side-stream gas sampling. PetCo2 measurements are dependent on tidal volume size because the exhaled gas has to carry alveolar gas. Deoxygenated Hb absorbs more red light and less infrared light than oxygenated Hb. As Sao2 increases, the ratio of the absorption of red light to that of infrared light decreases. It is assumed that in the circulation, changes in this ratio can only be produced by pulsating arterial blood. In neonates, Spo2 has been shown to correlate well with measured saturation in arterial samples (Hay et al, 1989). The absorption by pulsatile blood is only a small fraction of the light absorbed by tissue and venous blood. The accuracy of Spo2 is also affected by conditions such as low perfusion or by inappropriate placement such as excessive tightening of the probe (Bucher et al, 1994). Data indicate reliable detection of hypoxemia spells by pulse oximetry (Bohnhorst et al, 2000; Hay et al, 2002). Nonetheless, some hypoxemia episodes detected by pulse oximetry are considered artifactual because of their temporal association with infant movement. However, increased infant activity leading to heart rate, lung volume, and ventilation changes has been shown to trigger hypoxemia (Bolivar et al, 1995; Dimaguila et al, 1997) with increased frequency during periods when the infants are awake compared to periods of active or quiet sleep (Lehtonen et al, 2002). The preterm infant is at risk for O2-induced injury because of an immature antioxidant system that is unable to balance the oxidative effects of O2 radicals. In the past, severe neonatal lung injury was only partly attributed to exposure to high Fio2. However, animal experiments have showed that lung damage was caused by high alveolar O2 independent of Pao2 (Miller et al, 1970; Northway et al, 1967; Taghizadeh and Reynolds, 1976). In preterm infants, hyperoxia has been linked to neurologic damage and impairment (Ahdab-Barmada et al, 1980; Collins et al, 2001; Haynes et al, 2003). For this reason, when supplemental O2 is administered to hypoxemic neonates, oxygenation is continuously monitored to avoid hyperoxemia. Depending on the severity and duration of hypoxemia and the metabolic demands for oxygen, this can lead to reduced O2 availability and tissue hypoxia. Hypoxemia in the neonate can result from reduced alveolar oxygen content, low ventilation-perfusion ratio, reduced diffusion capacity, and extrapulmonary right-to-left shunts. The most common form of respiratory therapy for the neonate with hypoxemia consists of oxygen supplementation. The resulting increase in the alveolar-arterial O2 gradient (A-aDo2) in part compensates for the conditions producing hypoxemia mentioned earlier. The proportion of neonates requiring supplemental O2 increases with lower gestational ages because premature birth is associated with many of the factors that contribute to hypoxemia.