General Information about Trileptal
One of the primary benefits of Trileptal is its long-lasting impact. It is often taken twice a day, and unlike some other anticonvulsant medicines, it could provide steady and consistent seizure control without frequent dosage changes. This makes it a convenient option for patients to handle their epilepsy.
Trileptal works by stabilizing the electrical exercise in the mind, stopping or reducing the incidence of seizures. It does this by blocking the sodium channels in the brain, decreasing the abnormal electrical exercise that leads to seizures. It is very effective in treating focal seizures, which originate in a selected a half of the brain.
However, as with all medication, there are some precautions and potential dangers related to Trileptal. It could interact with other drugs, together with birth control tablets, and should cause delivery defects if taken during being pregnant. It is essential to consult with a healthcare professional earlier than starting or stopping any medicines.
Trileptal is also thought of to have a favorable safety profile compared to different anticonvulsants. It is usually well-tolerated and has a lower threat of great side effects. In clinical trials, the commonest unwanted facet effects reported had been dizziness, drowsiness, and fatigue. These unwanted facet effects are often gentle and often subside over time with continued use.
Epilepsy is a neurological disorder that impacts tens of millions of people around the world. It is characterised by recurring seizures, which are sudden bursts of electrical activity in the brain. These seizures can range from gentle to extreme and may greatly impact a person's quality of life. Thankfully, there are drugs available to help manage and control seizures. One such treatment is Trileptal.
Trileptal, additionally identified by its generic name oxcarbazepine, is an anticonvulsant medicine primarily used for the therapy of epilepsy. It was first accredited by the Food and Drug Administration (FDA) in 2000 and has since turn into a commonly prescribed medicine for those with seizure problems.
Trileptal is out there in pill or liquid kind, and the dosage is predicated on the patient's age, weight, and medical situation. It is important to follow the prescribed dosage and not to cease taking it without consulting a well being care provider, as all of a sudden stopping can increase the risk of seizures.
In conclusion, Trileptal is an efficient and handy medicine for the therapy of epilepsy. It is well-tolerated, has a long-lasting impact, and can be used for other situations. With correct management and common monitoring, Trileptal can significantly enhance the quality of life for these dwelling with epilepsy. However, it is essential to focus on any considerations or potential dangers with a healthcare skilled before starting this treatment.
In addition to its main use for controlling seizures, Trileptal has additionally been discovered to be efficient in managing different situations similar to bipolar disorder and neuropathic ache. It has been used off-label for these situations, and while extra analysis is required, the outcomes have been promising.
The dominant cells are clear 5 medications post mi trileptal 300 mg buy on line, lipid rich like the zona fasciculata and arranged in cords or alveoli. If bilateral nodular adrenal hyperplasia causes Conn syndrome, adrenals contain yellow cortical nodules, usually less than 2 cm. Polyuria and polydipsia result from impaired renal concentrating capacity, probably due to hypokalemia. Primary aldosteronism caused by an adenoma is curable by surgical removal of the tumor. Dietary sodium restriction and treatment with the aldosterone antagonist spironolactone are also frequently effective. Histogenesis of tumors of the adrenal medulla and extra-adrenal sympathetic nervous system. These cells are also present at extra-adrenal sympathetic nervous system sites, such as the preaortic sympathetic plexuses and paravertebral sympathetic chain. Chromaffin cells appear as nests of small polyhedral cells with pale amphophilic cytoplasm and vesicular nuclei. The cells of the adrenal medulla have many electron-dense, 100300-nm chromaffin (catecholamine-containing) granules, resembling those of sympathetic nerve endings. Epinephrine accounts for 85% of the content of these granules, with the remainder being norepinephrine and other noncatecholamine hormones. Interspersed among the chromaffin cells are postganglionic neurons and small autonomic nerve fibers. Stored catecholamines are secreted on sympathetic stimulation as a response to stress (exercise, cold, fasting, trauma) or emotional excitation accompanying fear and anger. The adrenal medulla is supplied by arterial and portal venous circulations that originate in the zona reticularis of the cortex. Most of the blood to the hormonally active cells of the medulla is from the portal system. The medulla is innervated from the splanchnic nerves by cholinergic preganglionic sympathetic neurons. If detected early, they are amenable to surgical resection, but if left untreated, patients can die of complications of prolonged hypertension. Most pheochromocytomas are unexpected findings at autopsy, indicating that some curable cases of hypertension escaped clinical detection. The pancreatic tumors tend to be multicentric and more malignant than in sporadic cases. Most (2/3) patients have adenomas of two or more endocrine organs, and 20% develop tumors of three or more. This gene encodes a nuclear protein, menin, which is thought to interact with the transcription factor junD. Mucosal neuromas are always present, but only half of patients express the full phenotype. Just as C-cell hyperplasia precedes medullary thyroid carcinomas, adrenal medullary hyperplasia may precede pheochromocytomas in these cases. Chromaffin cells are larger than normal and are arranged in distinct nests or cords. Typically, circumscribed nests (zellballen) of polyhedral to fusiform neoplastic cells contain granular, amphophilic or basophilic cytoplasm and vesicular nuclei. Electron microscopy shows membrane-bound, dense core granules, corresponding to stored catecholamines. The cut surface of an adrenal tumor from a patient with episodic hypertension is reddish brown with a prominent area of fibrosis. A photomicrograph of the tumor shows polyhedral tumor cells with ample finely granular cytoplasm. Many of the tumor cells show positive immunohistochemical staining for chromogranin A, a marker of neuroendocrine differentiation. Patients may come to medical attention because of (1) asymptomatic hypertension discovered on routine physical examination; (2) symptomatic hypertension resistant to antihypertensive therapy; (3) malignant hypertension. Typically, episodic catecholamine release leads to paroxysms or crises, of up to several hours, with severe throbbing headache, sweating, palpitations, tachycardia, abdominal pain and vomiting. Paroxysms can be triggered by activities that place pressure on the abdominal contents (including the tumor), such as exercise, lifting, bending or vigorous abdominal palpation. Episodic hypertension may become sustained and evolves into malignant hypertension in many untreated patients. Orthostatic hypotension results from decreased plasma volume and poor postural tone. Increased basal metabolism, sweating, heat intolerance and weight loss may mimic hyperthyroidism. The cardiac complications reflect myocardial necrosis caused by elevated catecholamine levels (catecholamine cardiomyopathy). Interestingly, carotid body tumors are 10-fold more common in people living at high altitude than in those at sea level, suggesting that these tumors reflect hyperplastic responses to prolonged carotid body sensing of hypoxia. Autosomal dominant transmission of paragangliomas occurs in some families, and hereditary paraganglioma was the first hereditary tumor syndrome reported to be caused by a germline mutation in a gene encoding a mitochondrial protein. All affected patients, whether male or female, inherit the disease from their fathers. Those genetically predisposed to this disease usually have multifocal tumors at an early age and follow autosomal dominant inheritance.
In these patients medications and breastfeeding trileptal 600 mg buy otc, iron is concentrated principally in mononuclear phagocytes, and cirrhosis is rare. In this setting, elevated hepcidin concentrations may severely restrict ferroportin function. This could impair iron absorption in the gut and lead to excessive iron retention in stores due to inadequate release from macrophages and hepatocytes. If hepcidin remains elevated for prolonged periods of time, iron deficiency anemia may develop. Thus, anemia in some chronic inflammatory diseases, such as Crohn disease and rheumatoid arthritis, or in some tumors, such as certain lymphomas, may be associated with anemia and high circulating hepcidin levels. Such anemias, although they show low blood iron levels, are not amenable to treatment with dietary iron, as high hepcidin levels impede enteric iron absorption. One in 150180 people is a carrier, and 1 in 30,000 children develop clinical disease. Copper is normally bound to ceruloplasmin in hepatocytes and then secreted into the blood. Kidneys (glomerluar and tubular dysfunction) A Footnote to Hepcidin-Regulated Iron Metabolism the centrality of hepcidin to iron metabolism may have implications far beyond hereditary iron storage disorders. As mentioned above, in chronic renal failure, the inability of the kidneys to eliminate hepcidin may lead to its accumulation. Most patients are compound heterozygotes and possess two different mutant alleles. Excess copper is toxic to hepatocytes, which die and release their copper into the blood, to then deposit in extrahepatic tissues. Copper can replace iron in the Fenton reaction to convert hydrogen peroxide into hydroxyl radicals (see Chapter 1). The deposition of copper in the Descemet membrane is reflected in a peripheral brown color, which obstructs the view of the underlying iris. Initial symptoms reflect chronic liver disease in about 1/2 of patients, 1/3 are first seen with neurologic complaints and about 1/10 have psychiatric illnesses. Eventually, chronic hepatitis and cirrhosis result in jaundice, portal hypertension and hepatic failure. If untreated, dysarthria and dysphagia appear, then disabling dystonia and spasticity. In some patients, these rings are accompanied by "sunflower cataracts," which are green copper discs in the anterior capsule of the lens. Copper-chelating agents, trientine and d-penicillamine, augment urinary copper excretion. Presymptomatic patients are maintained with zinc, which blocks intestinal absorption of copper. In patients who survive to adolescence, liver involvement becomes clinically symptomatic in 15%. Although it occurs in 1 of 2000 live births, only 10%15% of those affected develop liver disease. Most infants recover within 6 months, but 10%20% develop permanent liver disease. Children with cirrhosis usually die before 10 years of age from hepatic failure or other complications of the disease. Some patients are asymptomatic until early adulthood, when symptoms of cirrhosis may be the initial complaint. Insoluble aggregates of the mutant protein cannot be exported and accumulate, thereby damaging the cell. Micronodular cirrhosis develops by the age of 23 years in these children and may ultimately become macronodular. Of infants with Inborn Errors of Carbohydrate Metabolism Affect the Liver Glycogen Storage Diseases the biochemical basis of glycogen storage diseases is discussed in Chapter 6. The hepatocyte appearance with abundant glycogen is similar to glycogenosis type I. Deposits of mutant glycogen are also found in the heart, skeletal muscle and brain. Galactosemia Galactosemia is an autosomal recessive trait in which galactose-1-phosphate uridyl transferase is lacking. Affected infants who are fed milk rapidly develop hepatosplenomegaly, jaundice and hypoglycemia. Within 2 weeks of birth, the liver shows extensive and uniform fat accumulation and striking bile ductule proliferation in and around portal tracts. In fact, drugs are the most common cause of acute liver failure in the United States. Chapter 1 includes a discussion of mechanisms by which toxins may produce liver necrosis. The latter reflects injury that can occur with low frequency, irrespective of dose and without obvious predisposition (idiosyncratic reaction). The defining characteristics of predictable drug-induced hepatoxicity are: canaliculi and bile ductules. At about 6 weeks of age, fibrosis begins to extend from portal tracts into the lobules and progresses to cirrhosis by 6 months.
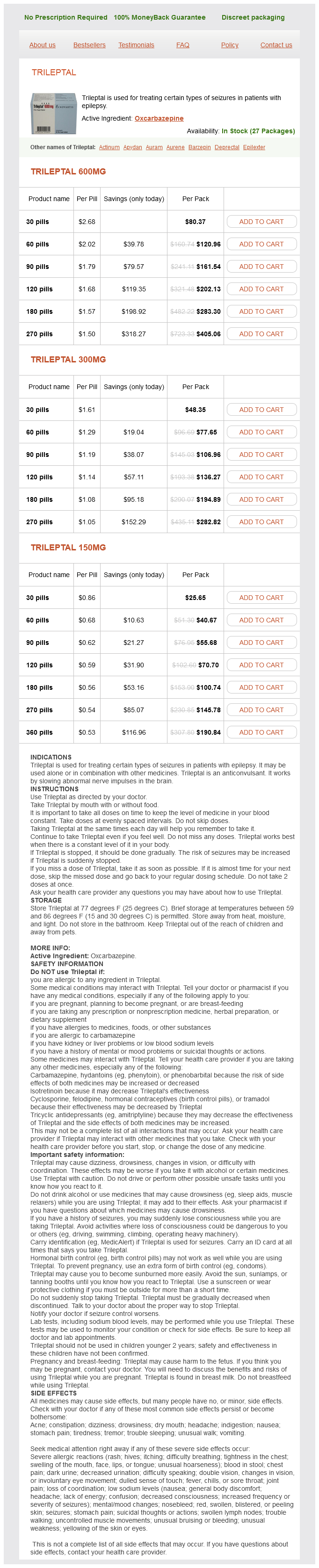
Trileptal Dosage and Price
Trileptal 600mg
- 30 pills - $80.37
- 60 pills - $120.96
- 90 pills - $161.54
- 120 pills - $202.13
- 180 pills - $283.30
- 270 pills - $405.06
Trileptal 300mg
- 30 pills - $48.35
- 60 pills - $77.65
- 90 pills - $106.96
- 120 pills - $136.27
- 180 pills - $194.89
- 270 pills - $282.82
Trileptal 150mg
- 30 pills - $25.65
- 60 pills - $40.67
- 90 pills - $55.68
- 120 pills - $70.70
- 180 pills - $100.74
- 270 pills - $145.78
- 360 pills - $190.84
Bleeding into the pericardial space caused by aggressive infectious or neoplastic processes or coagulation defects leads to hemorrhagic pericarditis symptoms 0f food poisoning trileptal 600 mg purchase free shipping. The heart of a patient who died in uremia displays a shaggy, fibrinous exudate covering the visceral pericardium. The pericardial space becomes obliterated, and visceral and parietal layers become fused in a dense, rigid mass of fibrous tissue. The condition is uncommon today and, in developed countries, is predominantly idiopathic. Prior radiation therapy to the mediastinum and cardiac surgery account for more than 1/3 of cases. Tuberculosis today accounts for fewer than 15% of cases of constrictive pericarditis in industrialized countries, but it is still the major cause in underdeveloped regions. These differ from the pain of angina pectoris or myocardial infarction by their failure to radiate down the left arm. Electrocardiographic changes reflect repolarization abnormalities of the myocardium. Idiopathic or viral pericarditis is a self-limited disorder, but it may infrequently lead to constrictive pericarditis. These patients have high venous pressure, low cardiac output, small pulse pressure and fluid retention with ascites and peripheral edema. Adhesive pericarditis is a much milder form of healing of an inflamed pericardium. Internal mammary artery grafts develop fewer pathologic changes and so last longer than vein grafts. Excised saphenous vein segments used as grafts are subjected to unavoidable surgical manipulation and an interval of ischemia during harvesting, which injures endothelial cells. Grafted veins are also exposed to arterial pressures that are much higher than those in their native location. Finally, the caliber of the vein, which is expanded by arterial blood pressure, is usually much greater than that of the distal coronary artery at the graft anastomosis, and this mismatch promotes blood stasis. In the immediate postoperative period, these factors enhance the chance of thrombosis and probably eventually lead to intimal hyperplasia. Intimal hyperplasia is a concentric increase of smooth muscle cells, fibroblasts and collagen in the intima of the vein. After several years, lipids may deposit and atherosclerotic plaques may form in the thickened intima of vein grafts. Atherosclerosis is the most frequent cause of vein graft failure in patients who have had good graft function for several years after surgery. Since arteries are better aortocoronary bypass conduits than veins, some surgeons have developed total arterial bypass procedures that use internal mammary, radial and selected abdominal arteries that can be taken without endorgan damage. The pericardial space has been obliterated, and the heart is encased in a fibrotic, thickened pericardium. Tissue Xenografts and Mechanical Valves Typically Are Used to Replace Damaged Cardiac Valves In most patients with severe valve dysfunction, valve replacement is the best prospect for long-term symptomatic improvement. Operative mortality is low, especially for patients with good preoperative myocardial function. Half of all patients with prosthetic valves are free of complications after 10 years. These valves have good hemodynamic characteristics, cause little obstruction and resist thromboembolic complications. The most common cause of failure of tissue-valve prostheses is tissue degeneration with calcification and fragmentation of prosthetic valve cusps. This developed within 5 years of implantation in virtually all early-generation porcine aortic valves and led to valve failure in 20%30% of patients within 10 years. Improved understanding of prosthetic tissue-valve calcification has led to development of anticalcification treatments that improve valve longevity and performance. Tissue-valve calcification occurs mainly within residual cells killed by glutaraldehyde treatment. Strategies to prevent or delay such calcification include removal of residual cells, binding of calcification inhibitors to the glutaraldehyde-fixed tissue and use of other tissue cross-linking and preservation reagents. However, the risk of thromboembolism makes long-term anticoagulant therapy imperative. A catheter with a deflated balloon covered by a collapsed cylindrical metallic mesh (stent) is positioned in the stenotic segment. As the stent deploys, it holds the fragmented wall open and keeps the vessel lumen patent. Most patients receive drug-eluting stents, which slowly release antiproliferative agents such as everolimus or paclitaxel. Coronary Bypass Grafts Circumvent Obstructed Segments Coronary bypass grafting, using a saphenous vein or left internal mammary artery to redirect blood around a blockage, is common treatment for proximal coronary stenosis. Although operative mortality is low and early symptomatic relief occurs in most patients, myocardial perfusion is not permanently improved, owing to several complications: (1) early thrombosis, (2) intimal hyperplasia and (3) atherosclerosis of vein grafts. An endomyocardial biopsy shows lymphocytes surrounding individual myocytes and expanding the interstitium. An intramyocardial branch of a coronary artery shows prominent intimal proliferation and inflammation with concentric narrowing of the lumen. Cancer Survivors May Experience Long-Term Cardiovascular Complications As more patients survive cancer chemotherapy and/or radiation therapy, increased rates of cardiovascular disease attributable to their therapy are becoming recognized. Radiation also contributes to pericardial disease, cardiomyopathy and valvular dysfunction. Heart Transplantation May Cure Many End-Stage Heart Diseases but Is Subject to Host Rejection Processes the development of effective immunosuppressive regimens and surveillance endomyocardial biopsy protocols has made cardiac transplantation an effective treatment for end-stage heart disease. Allograft rejection (see Chapter 4), however, is a major complication of cardiac transplantation.