General Information about Red Viagra
One of the main benefits of Red Viagra is its ability to offer long-lasting effects, as much as 4 hours after consumption. This gives males the boldness to have interaction in sexual actions without the worry of dropping their erection prematurely. It additionally allows them to have multiple periods in one night, tremendously enhancing their sexual experiences.
While the commonest cause of ED is the natural getting older process, other components such as stress, nervousness, melancholy, and certain medical conditions like diabetes, hypertension, and heart illness can also contribute to it. Red Viagra has been proven to be effective whatever the underlying reason for ED, making it a go-to medication for a lot of men.
Red Viagra, also called Sildenafil Citrate, is a phosphodiesterase kind 5 (PDE5) inhibitor, which implies it actually works by growing blood flow to the penis, helping men obtain and maintain an erection. It is identical lively ingredient discovered within the well-known blue capsule Viagra, but Red Viagra has the next dosage. This makes it more potent and allows it to ship quick and dependable results.
As with any treatment, there are potential side effects of using Red Viagra. These embrace complications, dizziness, flushing, upset abdomen, and modifications in imaginative and prescient. However, these unwanted aspect effects are usually delicate and short-term. In uncommon cases, more serious unwanted effects could happen, and if this occurs, you will want to search medical attention instantly.
Red Viagra is a well-known medication used for treating impotency among men. It is a powerful and effective drug that has been helping men all round the world regain their sexual confidence. With its stunning red color and unparalleled results, Red Viagra has turn out to be a popular alternative for men struggling with erectile dysfunction.
Red Viagra is obtainable in pill kind and should be taken orally with a glass of water. It is really helpful to take it 30 minutes to an hour before participating in sexual exercise. The dosage might range primarily based on an individual’s needs and overall well being. It is always advisable to consult a doctor to find out the suitable dosage and whether or not it is secure for you to use.
The brilliant red colour of Red Viagra isn't just for aesthetics, but it additionally represents the energy and vitality it provides. Its distinctive colour has earned it the nickname “the little red tablet.” And just like the well-known blue capsule, it has additionally gained a reputation for being a surprise drug for men’s sexual well being.
Erectile dysfunction (ED) is a condition the place a person is unable to get or keep an erection lengthy sufficient to have sexual intercourse. This could be a source of immense frustration and embarrassment for those affected by it. According to the National Institutes of Health, ED affects approximately 30 million men in the United States alone, and the numbers are even greater globally.
In conclusion, Red Viagra has become a game-changer within the therapy of ED, providing males with a protected and reliable solution to their sexual issues. Its daring pink color, efficiency, and effectiveness have made it a preferred alternative among shoppers. However, it's essential to keep in thoughts that it is a prescription medication and will solely be used under medical supervision to make sure security and effectiveness. With Red Viagra, men can as quickly as once more get pleasure from a healthy and satisfying sex life.
Large ulcers may require 2 to 3 weeks to heal erectile dysfunction studies generic 200 mg red viagra with visa, with clinical resolution of lymphadenopathy slower than that of ulcers. Approximately 10% of women whose ulcers initially heal have a recurrence at the same site. Syphilis Syphilis is a chronic, complex systemic disease produced by the spirochete Treponema pallidum. Even with mandatory screening, congenital syphilis continues to be a public health problem. Mothers who experience stillbirth or neonatal death from syphilis usually have not received prenatal care. Therefore the presence of spirochetes is diagnosed by use of specially adapted techniques, dark-field microscopy, or direct fluorescent antibody tests. They replicate every 30 to 36 hours, which accounts for the comparatively long incubation period. Approximately 3% to 10% of patients contract the disease from a single sexual encounter with an infected partner. Similar studies have documented that 30% of individuals become infected during a 1-month exposure to a sexual partner with primary or secondary syphilis. Patients are contagious during primary, secondary, and probably the first year of latent syphilis. Syphilis can be spread by kissing or touching a person who has an active lesion on the lips, oral cavity, breast, or genitals. The diagnosis of syphilis is complicated by the fact that the organism cannot be cultivated in vitro. There are two types of serologic tests, the nonspecific nontreponemal and the specific antitreponemal antibody tests. They are used as screening tests for the disease, typically become positive 4 to 6 weeks after exposure, and also are a useful index of treatment response. Quantitative nontreponemal antibody titers usually correlate with the activity of the disease. Serologic testing is an indirect method of diagnosis because it relies on a humoral immune response to infection. Approximately 1% of patients have technical or biologic false-positive results with the nonspecific tests. Biologic false-positive serum tests usually are associated with extremely low titers (<1:8). A false-negative result is a possibility, occurring in approximately 1% to 2% of tests. This negative reaction occurs in women in whom there is an excess of anticardiolipin antibody in the serum, termed the prozone phenomenon. Women with immunocompromise also may have false-negative tests because of their inability to produce the antibodies detected by these screening tests. If a nonspecific test result is positive, the significance of this result must be confirmed by a specific antitreponemal test. Antitreponemal tests are more sensitive; however, occasionally, they may produce false-positive results. A woman with a positive reactive treponemal test usually will have this positive reaction for her lifetime, regardless of treatment or activity of the disease. In primary syphilis, a papule, which is usually painless, appears at the site of inoculation 2 to 3 weeks after exposure. This soon ulcerates to produce the classic finding of primary syphilis, a chancre that is a painless ulcer, 1 to 2 cm, with a raised indurated margin and a nonexudative base. Usually, the chancre is solitary, painless, and found on the vulva, vagina, or cervix, although extragenital primary lesions, including lesions of the mouth, anal canal, and breast nipple, have been reported in approximately 5% of patients. Nontender and firm regional adenopathy is present during the first week of clinical disease. Hence, many women do not seek treatment, a feature that enhances the likelihood of transmission. Confirmation that the ulcer is primary or secondary syphilis depends on the identification of T. It is important to clean and abrade the ulcer with gauze before obtaining the serum for the slides. If the serologic test result remains negative for 3 months, it is unlikely that the ulcer was syphilis. If primary syphilis is untreated, approximately 25% of individuals develop secondary syphilis, which is the result of hematogenous dissemination of the spirochetes. Secondary syphilis is a systemic disease that develops between 6 weeks and 6 months (average, 9 weeks) after the primary chancre. Approximately 25% of women still have a primary chancre when the secondary lesions appear. An untreated attack of secondary syphilis will last 2 to 6 weeks, and a multitude of systemic symptoms may occur, depending on the major organs involved, such as rash, fever, headache, malaise, lymphadenopathy, and anorexia. The classic rash of secondary syphilis is red macules and papules over the palms of the hands and the soles of the feet. Vulvar lesions of condyloma latum are large, raised, flattened, grayish white areas. These ulcers are larger than herpetic ulcers and are not tender unless secondarily infected. A woman with syphilis is most infectious during the first 1 to 2 years of disease, with decreasing infectivity thereafter.
Postmenopausal Bartholin gland enlargement: a hospitalbased cancer risk assessment erectile dysfunction 16 red viagra 200 mg mastercard. Clinical predictors for buserelin acetate treatment of uterine fibroids: a prospective study of 40 women. Uterine artery embolization for symptomatic fibroids: clinical results in 400 women with imaging follow up. Acute changes in endometrial thickness after aspiration of functional ovarian cysts. Vaginal fibromyomata: two cases with preoperative assessment, resection, and reconstruction. The wide spectrum of clinical problems that occur with endometriosis has frustrated gynecologists, fascinated pathologists, and burdened patients for years. Although endometriosis was first described in 1860, the classic studies by Sampson in the 1920s were the first to emphasize the clinical and pathologic correlations of endometriosis (Sampson, 1927). By definition, endometriosis is the presence and growth of the glands and stroma of the lining of the uterus in an aberrant or heterotopic location. Adenomyosis is the growth of endometrial glands and stroma into the uterine myometrium to a depth of at least 2. Adenomyosis is sometimes termed internal endometriosis; however, this is a semantic misnomer because most likely they are separate diseases. It is usually stated that the incidence of endometriosis has been increasing since the 1980s. This opinion is secondary to an enlightened awareness of mild endometriosis as diagnosed by the increasing use of laparoscopy. Since the early 2000s, diagnostic delay, the average time to the first diagnosis of the disease, has decreased dramatically. Evers has advanced a provocative hypothesis that endometrial implants in the peritoneal cavity are a physiologic finding secondary to retrograde menstruation, and their presence does not confirm a disease process (Evers, 1994). The overall prevalence of endometriosis in reproductive aged women has been suggested to be as high as 11% (Buck Louis, 2011). The age-specific incidence or prevalence of endometriosis is not known and has only been estimated. Many patients are diagnosed incidentally during surgery performed for a variety of other indications. Conservative estimates find that endometriosis is present in 5% to 15% of laparotomies performed on reproductive-age females. The prevalence of active endometriosis is approximately 33% in women with chronic pelvic pain. In a compilation of eight studies encompassing 162 patients with endometriosis, the natural course of endometriosis has been reported to increase or progress 31% of the time, to remain the same 32% of the time and to regress in 38% (Taylor, 2014). The cause of endometriosis is uncertain and involves many mechanisms including retrograde menstruation, vascular dissemination, metaplasia, genetic predisposition, immunologic changes, and hormonal influences, as discussed later. In addition, there is increasing evidence that environmental factors may also play a role, including exposure to dioxin and other endocrine disruptors. Clinically, it is most difficult to predict the natural course of endometriosis in any one individual. For example, the clinician cannot know which woman with mild disease in her 20s will progress to severe disease at a later age. The typical patient with endometriosis is in her mid-30s, is nulliparous and involuntarily infertile, and has symptoms of secondary dysmenorrhea and pelvic pain, but it must be stressed that symptoms and signs may be extremely variable. Aberrant endometrial tissue grows under the cyclic influence of ovarian hormones and is particularly estrogen dependent; therefore, the disease is most commonly found during the reproductive years. Endometriosis in teenagers should be investigated for obstructive reproductive tract abnormalities that increase the amount of retrograde menstruation. Although previously thought to be rare in adolescents, in teens with pelvic pain, endometriosis has been found in approximately half the cases. Endometriosis is a disease not only of great individual variability but also of contrasting pathophysiologic processes. It is a benign disease, yet it has the characteristics of a malignancy- that is, it is locally infiltrative, invasive, and widely disseminating. Although the physiologic levels of estrogen stimulate the growth of ectopic endometrium, the use of contraceptive steroids of various doses is usually beneficial for treatment. Another contrast often noted is the inverse relationship between the extent of pelvic endometriosis and the severity of pelvic pain. Women with extensive endometriosis may be asymptomatic, whereas other patients with minimal implants may have incapacitating chronic pelvic pain. However, as would be expected, women with deep infiltrating endometriosis, especially in retroperitoneal spaces, often experience severe episodes of pain. The clinical variability in responses among women with endometriosis may relate to differences in immunologic function and variations in cytokine production. However, no single theory adequately explains all the manifestations of the disease. Most important, there is only speculation as to why some women develop endometriosis and others do not. Retrograde Menstruation the most popular theory is that endometriosis results from retrograde menstruation. Sampson suggested that pelvic endometriosis was secondary to implantation of endometrial cells shed during menstruation (Sampson, 1927). It has been suggested that the shedding of endometrial-based adult stem cells and mesenchymal cells may explain this phenomenon (Gargett, 2010). These cells attach to the pelvic peritoneum and under hormonal influence grow as homologous grafts.
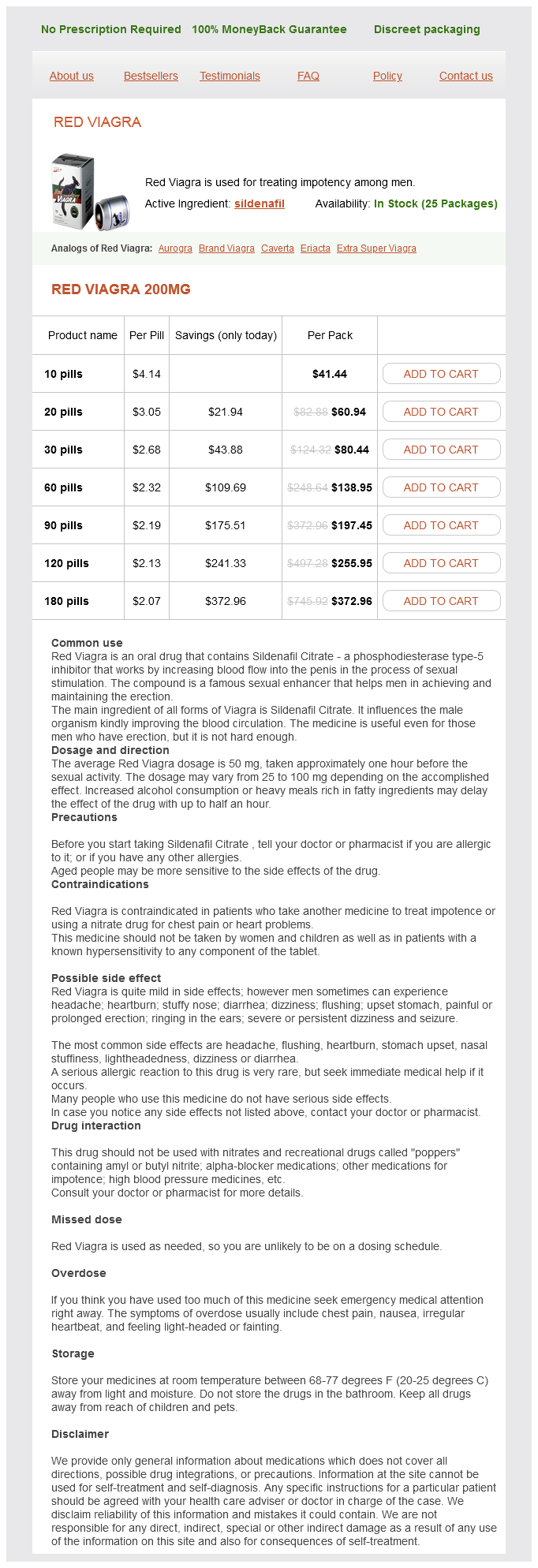
Red Viagra Dosage and Price
Red Viagra 200mg
- 10 pills - $41.44
- 20 pills - $60.94
- 30 pills - $80.44
- 60 pills - $138.95
- 90 pills - $197.45
- 120 pills - $255.95
- 180 pills - $372.96
C erectile dysfunction ear order red viagra 200 mg with visa, Small cell neuroendocrine carcinoma of the cervix (arrow) infiltrating between normal endocervical glands (H&E, × 240). Glands are mostly well differentiated, appearing normal except for their irregular shapes. Glandular structure lies adjacent to a nest of nonkeratinizing large squamous cells (× 400). Adenosquamous carcinomas, as the name implies, consist of squamous carcinoma and adenocarcinoma elements in varying proportions. This is an undifferentiated tumor consisting of large cells containing cytoplasm, with a ground-glass appearance. Glassy cell carcinomas tend to metastasize early to lymph nodes as well as to distant sites and usually have a fatal outcome. Small cell carcinoma of the cervix is rare, comprising less than 5% of all carcinomas of the cervix. Women with small cell carcinoma are likely to be 10 years younger than those with squamous cell carcinoma. They behave aggressively and are frequently associated with widespread metastasis to multiple sites, including bone, liver, skin, and brain. Efforts to treat these cancers with approaches typically used for small cell carcinoma of the lung have had mixed results. These tumors contain intermediate to large cells, high-grade nuclei, and eosinophilic cytoplasmic granules of the type seen in neuroendocrine cells. Reported survival rates for patients with these aggressive carcinomas are similar to those of patients with small cell tumors, and optimal therapy has yet to be established. Cells have sharp borders, ground-glasstype cytoplasm, and nuclei containing prominent nucleoli (× 1000). These patients often have a history of not having had a cytologic (Pap) smear for many years. Other symptoms, such as back pain, loss of appetite, and weight loss, are late manifestations and occur when there is extensive spread of cervical carcinoma. Preinvasive intraepithelial carcinoma of the cervix (see Chapter 28) occurs primarily in women in their 20s and 30s and has become more common in those in their 20s, leading to a gradual increase in the incidence of invasive carcinoma in younger patients. The diagnosis is established by biopsy of the tumor; a specimen can easily be obtained during an office examination. A Kevorkian, Eppendorf, Tischler, or similar punch biopsy instrument is convenient to use. Occasionally, it is necessary to biopsy nodularity or indurations in the vagina near the cervix to ascertain the limit of tumor spread and define a correct tumor stage. All cases with hydronephrosis or a nonfunctioning kidney are included, unless they are known to be from another cause. Invasion is limited to a measured stromal invasion, with a maximum depth of 5 mm and a horizontal extension of not >7 mm. Depth of invasion should not be >5 mm taken from the base of the epithelium of the original tissue, superficial or glandular. The depth of invasion should always be reported in millimeters, even in those cases with early (minimal) stromal invasion (minus 1 mm). The involvement of vascular or lymphatic spaces should not change the stage allotment. On rectal examination, there is no cancer-free space between the tumor and the pelvic wall. Alternatively, they may be endophytic, in which case they are asymptomatic, particularly in the early stage of development, and tend to be deeply invasive when diagnosed. These usually start initially from an endocervical location and often fill the cervix and lower uterine segment, resulting in a barrel-shaped cervix. The latter tumors tend to metastasize to regional pelvic nodes and, because of the tendency of late diagnosis, are often more advanced than the exophytic variety. Rarely, the inguinal nodes are involved; however, if the lower third of the vagina is involved, the median inguinal nodes should be considered a primary node. The distribution of lymph node involvement in 26 cases of untreated carcinoma of the cervix was studied in detail by Henriksen. The obturator lymph nodes were the most frequently involved, with a rate of 19% (39 of 208), and the authors proposed them as sentinel nodes for cervical cancers. An important distal node that becomes involved after the paraaortic group is the left scalene node-that is, the left supraclavicular node. A biopsy of this node may be performed in the assessment of advanced cervical carcinoma to clarify whether the tumor has spread outside the abdomen. In addition to nodal spread, hematogenous spread of cervical carcinoma occurs primarily to the lung, liver and, less frequently, bone (see Recurrence later in the chapter). One of the most important predictors is tumor size for local recurrence and death for patients treated with surgery or radiation therapy (Eifel, 1994). Another important prognostic factor is involvement of lymph nodes, which also is not part of the clinical staging system. In several surgical series, after a radical hysterectomy, patients with positive pelvic lymph nodes had a 35% to 40% lower 5-year survival rate than patients with negative nodes. Bloodborne metastases from cervical carcinomas do occur but are less frequent and are usually seen late in the course of the disease. Initially, cervical carcinoma spreads to the primary pelvic nodes, which include the pericervical node; presacral, hypogastric (internal iliac), and external iliac nodes; and nodes in the obturator fossa near the vessels and nerve. From this primary Obstetrics & Gynecology Books Full 29 Malignant Diseases of the Cervix 671 Distant metastases 27% A B Aortic 27% Common iliac 31% Sacral 23% C D Paracervical 31% Hypogastric 31% Ext.