General Information about Myambutol
In conclusion, Myambutol is a vital part within the remedy of TB infections of the lung. It is a broadly used and effective medicine that has been serving to patients battle this disease for decades. When used together with other TB medication, Myambutol can significantly enhance the chances of curing TB and stopping its unfold to others. However, it is important to follow the prescribed remedy plan and report any side effects to a healthcare supplier promptly. With correct use and adherence, Myambutol can continue to play a vital position in the struggle in opposition to TB and help save countless lives.
Myambutol was first introduced in the Nineteen Sixties and has been used successfully for the therapy of TB ever since. It is out there within the form of oral tablets and is often taken as soon as a day. The dosage and period of remedy will depend on the severity of the an infection and the affected person's total well being.
It is worth noting that Myambutol ought to at all times be utilized in mixture with different TB medications. This is as a result of using only one medicine can result in the event of drug-resistant TB strains. When used appropriately, Myambutol can successfully kill the bacteria responsible for TB and stop its spread to others.
As with all antibiotics, it's essential to finish the prescribed course of therapy for Myambutol to be efficient. Stopping the treatment early can outcome in a relapse of TB, and the bacteria can turn out to be proof against the drug, making it more difficult to deal with in the future.
Tuberculosis, or TB, is a serious bacterial infection that primarily impacts the lungs. It is a highly contagious illness that could be unfold through the air when an infected individual coughs, sneezes, or speaks. According to the World Health Organization, TB is doubtless certainly one of the high ten causes of dying worldwide, with an estimated 1.4 million fatalities in 2019 alone. Thankfully, with the event of contemporary drugs, TB is now a treatable and curable illness, and one of the drugs utilized in its therapy is Myambutol.
Myambutol, additionally known by its generic name, ethambutol, is an antibiotic generally used in mixture with other drugs to deal with TB infections of the lungs. It works by stopping the growth of micro organism, allowing the body's immune system to struggle off the an infection.
Like any medicine, Myambutol could cause unwanted side effects, although not everybody experiences them. The most commonly reported unwanted aspect effects embody nausea, vomiting, lack of appetite, and joint pain. In some circumstances, Myambutol can cause vision problems, such as blurred imaginative and prescient and issue distinguishing the colors green and purple. Therefore, anyone taking Myambutol should endure regular eye check-ups.
One of the distinctive features of Myambutol is its capacity to deal with TB attributable to drug-resistant bacteria. Multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB) are becoming increasingly prevalent, posing a major challenge for world TB management efforts. Myambutol, along with other TB drugs, is essential in treating these type of TB infections, that are more difficult and expensive to handle.
Both ketorolac and diclofenac are effective in treating cystoid macular edema occurring after cataract surgery and in controlling pain after corneal refractive surgery infection xbox 360 buy myambutol 800 mg cheap. Bromfenac and nepafenac are indicated for treating postoperative pain and inflammation after cataract surgery. Postoperative ocular inflammation; uveitis; vernal keratoconjunctivitisa Rimexolone a 1% suspension Off-label use. H1 antagonists (see Chapter 32) and mast cell stabilizers are used to treat the manifestations of ocular allergies. Cromolyn sodium has found some use in treating conjunctivitis that is thought to be allergen mediated, such as vernal conjunctivitis. The mast cell stabilizer lodoxamide tromethamine is available for ophthalmic use for the treatment of ocular inflammatory states such as vernal conjunctivitis and keratitis. Nedocromil, primarily a mast cell stabilizer with some antihistaminic properties, is also used. Likewise, olopatadine hydrochloride, ketotifen fumarate, bepotastine, Antihistamines and Mast Cell Stabilizers azelastine, and alcaftadine are H1 antagonists with mast cellstabilizing properties. Epinastine antagonizes H1 and H2 receptors and exhibits mast cellstabilizing activity. Topical cyclosporine (Table 6912) is approved for the treatment of chronic dry eye associated with inflammation. Use of cyclosporine is associated with decreased inflammatory markers in the lacrimal gland, increased tear production, and improved vision and comfort. Topical lifitegrast (Table 6912) is approved to treat the signs and symptoms of dry eye disease. Interferon 2b is used off label in the treatment of conjunctival papilloma and certain conjunctival tumors. Fibrin sealants are increasingly being used on the ocular surface to secure tissue such as conjunctiva, amniotic membrane, and lamellar corneal grafts. Similarly, these gases can be used after endothelial keratoplasty to help the lamellar graft adhere to the posterior cornea. Mitomycin is used intraoperatively as a single sub- conjunctival application at the trabeculectomy site. Both agents work by limiting the healing process; sometimes this can result in thin, ischemic, avascular tissue that is prone to breakdown. Mitomycin can be used to reduce the risk of scarring after procedures to remove corneal opacities and prophylactically to prevent corneal scarring after photorefractive and phototherapeutic keratectomy. Mitomycin also is used to treat certain conjunctival and corneal tumors and to decrease recurrence after pterygium excision. Caution is advocated when using mitomycin in light of the potentially serious delayed ocular complications. Vitreous Substitutes Agents Used in Ophthalmic Surgery Presurgical Antiseptics Povidone iodine is formulated as a 5% sterile ophthalmic solution for use prior to surgery to prepare periocular skin and irrigate ocular surfaces, including the cornea, conjunctiva, and palpebral fornices. Several compounds, including gases, perfluorocarbon liquids, and silicone oils, are available as vitreous substitutes (Table 6913). Their primary use is reattachment of the retina following vitrectomy and membrane-peeling procedures for complicated proliferative vitreoretinopathy and traction retinal detachments. The gases are absorbed over a period of days (for air) to 2 months (for perfluoropropane). Silicone oil (polydimethylsiloxanes) is used for long-term tamponade of the retina. Complications from silicone oil use include glaucoma, cataract formation, corneal edema, corneal band keratopathy, and retinal toxicity. Viscoelastic Substances Surgical Hemostasis and Thrombolytic Agents the viscoelastic substances are agents that assist in ocular surgery by maintaining spaces, moving tissue, and protecting surfaces. These substances are prepared from hyaluronate, chondroitin sulfate, or hydroxypropylmethylcellulose and share varying degrees of the following important physical characteristics: viscosity, shear flow, elasticity, cohesiveness, and coatability. Hemostasis has an important role in most surgical procedures and usually is achieved by temperature-mediated coagulation. Intravitreal administration of thrombin can assist in controlling intraocular hemorrhage during vitrectomy. When used intraocularly, a potentially significant inflammatory response may occur that can be minimized by thorough irrigation after hemostasis is achieved. With normal 1265 dosages, toxicity does not appear until about 6 years after the drug is started. Stopping the drug will not reverse the damage but generally will prevent further toxicity. The antiseizure drug vigabatrin causes progressive and permanent bilateral concentric visual field constriction in a high percentage of patients. Multiple medications, including ethambutol, chloramphenicol, and rifampin, can cause toxic optic neuropathy characterized by gradually progressive bilateral central scotomas and vision loss. If the steroids cannot be stopped, glaucoma medications, and even filtering surgery, often are required. Isotretinoin has a drying effect on mucous membranes and is associated with dry eye and severe dysfunction of the meibomian gland. Cornea, Conjunctiva, and Eyelids Botulinum Toxin Type A in the Treatment of Strabismus, Blepharospasm, and Related Disorders Two botulinum toxin type A preparations are marketed in the U.
Toxicity Chronic use of class 1 topical glucocorticoids can cause skin atrophy treatment for esbl uti generic 800 mg myambutol fast delivery, striae, telangiectasias, purpura, and acneiform eruptions. Pulse therapy using large intravenous doses of methylprednisolone sodium succinate is an option for severe resistant pyoderma gangrenosum, pemphigus vulgaris, systemic lupus erythematosus with multisystem disease, and dermatomyositis. More rapid infusion has been associated with increased rates of hypotension, electrolyte shifts, and cardiac arrhythmias. Toxicity and Monitoring Oral glucocorticoids have numerous systemic effects, as discussed in Chapter 46. Retinoids Retinoids comprise natural and synthetic compounds that exhibit vitamin A like biological activity or bind to nuclear receptors for retinoids. Characteristics of topical and systemic retinoids are summarized in Tables 704 and 705, respectively. Chronic administration of oral glucocorticoids is problematic, given the side effects associated with their long-term use (see Chapter 46). Daily morning dosing with prednisone generally is preferred, although divided doses occasionally are used to enhance efficacy. Side effects of systemic retinoids include dry skin, nosebleeds from dry mucous membranes, conjunctivitis, reduced night vision, hair loss, alterations in serum lipids and transaminases, hypothyroidism, inflammatory bowel disease flare, musculoskeletal pain, pseudotumor cerebri, and mood alterations. Because all oral retinoids are potent teratogens, they should be used carefully in females of childbearing potential and not in pregnant patients. Topical retinoids are first-line agents for noninflammatory (comedonal) acne and often are combined with other agents in the management of inflammatory acne. Fine wrinkles and dyspigmentation, two important features of photoaging, are also improved with topical retinoids. In the epidermis, retinoids induce epidermal hyperplasia in atrophic skin and reduce keratinocyte atypia. These effects often decrease with time and are lessened by concomitant use of emollients. Although there is little systemic absorption of topical retinoids and no alteration in plasma vitamin A levels with their use, topical retinoids are not recommended for use during pregnancy. Available Agents; Clinical Use Least potent 7 First-generation retinoids include retinol (vitamin A), tretinoin (all-trans-retinoic acid; vitamin A acid), isotretinoin (13-cis-retinoic acid), and alitretinoin (9-cis-retinoic acid). Third-generation retinoids were designed to optimize receptor-selective binding and include tazarotene, bexarotene, and adapalene. Both retinoid receptor families have three isoforms (, and), which are expressed in unique Tretinoin (all-trans-retinoic acid) is photolabile and should be applied once nightly for acne and photoaging. Benzoyl peroxide also inactivates tretinoin and should not be applied simultaneously. Formulations with copolymer microspheres or prepolyolprepolymer 2 that gradually release tretinoin to decrease irritancy are available and are less susceptible to oxidation by benzoyl peroxide and photodegradation. Adapalene has similar efficacy to tretinoin, but unlike tretinoin, it is stable in sunlight or the presence of benzoyl peroxide and tends to be less irritating. Tazarotene is approved for the treatment of psoriasis, photoaging, facial wrinkles, and acne vulgaris. Tazarotene gel, applied once daily, may be used as monotherapy or in combination with other medications, such as topical corticosteroids, for the treatment of localized plaque psoriasis. Topical corticosteroids improve the efficacy of therapy and reduce the side effects of burning, itching, and skin irritation that are commonly associated with tazarotene. Its application is titrated up from every other day to two to four times daily over several weeks to improve patient tolerance. Less common laboratory abnormalities include elevated transaminases, decreased thyroid hormone, and leukopenia. These laboratory values are usually subsequently checked monthly for the first 36 months and once every 3 months thereafter. In addition, two negative pregnancy tests on separate occasions are required for females of childbearing potential prior to starting acitretin or isotretinoin; bexarotene requires one negative pregnancy test within the week prior to initiating therapy. Therapeutic Uses and Contraindications Off-label uses include ichthyosis, Darier disease, pityriasis rubra pilaris, rosacea, hidradenitis suppurativa, chemoprevention of malignancy, lichen sclerosus, subacute lupus erythematosus, and discoid lupus erythematosus. Absolute contraindications include use by women who are pregnant, planning to become pregnant, or breastfeeding. Relative contraindications include leukopenia, alcoholism, hyperlipidemia, hypercholesterolemia, hypothyroidism, and significant hepatic or renal disease. Available Agents and Clinical Use Toxicity and Monitoring Acute toxicities may include mucocutaneous or laboratory abnormalities; bony changes may occur after chronic use at high doses. Mucocutaneous side effects may include cheilitis, xerosis, blepharoconjunctivitis, cutaneous photosensitivity, photophobia, myalgia, arthralgia, headaches, alopecia, nail fragility, and increased susceptibility to staphylococcal infections. Some patients develop a "retinoid dermatitis" characterized by erythema, pruritus, and scaling. Very rarely, patients may develop pseudotumor cerebri, especially when systemic retinoids are combined with tetracyclines. Isotretinoin is approved for the treatment of recalcitrant and nodular acne vulgaris. The drug has remarkable efficacy in severe acne and may induce prolonged remissions after a single course of therapy. Approximately one-third of patients will relapse, usually within 3 years of stopping therapy. Although most relapses are mild and respond to conventional management with topical and systemic antiacne agents, some may require a second course of isotretinoin. An isotretinoin-Lidose formulation (a eutectic mixture of drug and lipids in a hard gelatin capsule) may be given without respect to meals.
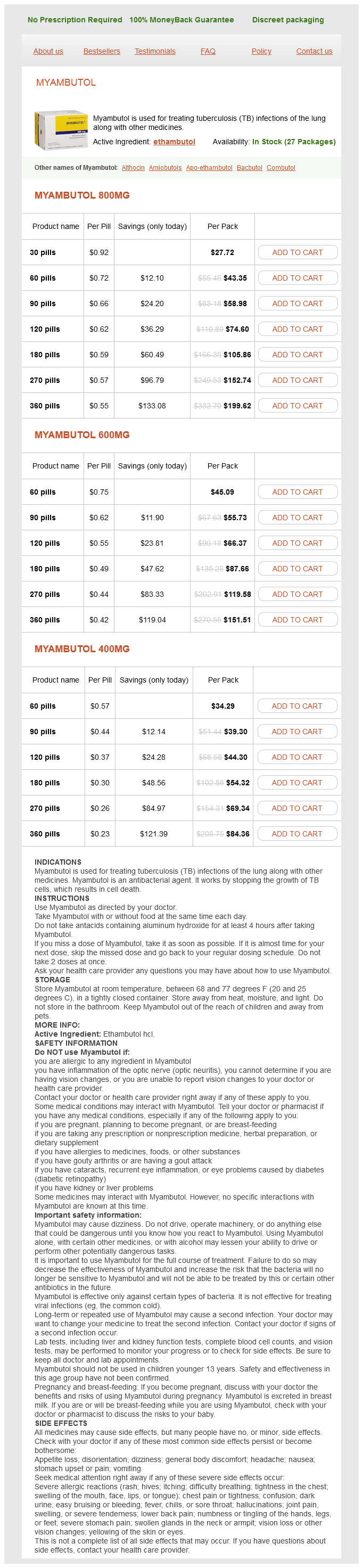
Myambutol Dosage and Price
Myambutol 800mg
- 30 pills - $27.72
- 60 pills - $43.35
- 90 pills - $58.98
- 120 pills - $74.60
- 180 pills - $105.86
- 270 pills - $152.74
- 360 pills - $199.62
Myambutol 600mg
- 60 pills - $45.09
- 90 pills - $55.73
- 120 pills - $66.37
- 180 pills - $87.66
- 270 pills - $119.58
- 360 pills - $151.51
Myambutol 400mg
- 60 pills - $34.29
- 90 pills - $39.30
- 120 pills - $44.30
- 180 pills - $54.32
- 270 pills - $69.34
- 360 pills - $84.36
Several groups then isolated progesterone from mammalian corpora lutea in the 1930s treatment for dogs bad breath generic myambutol 600 mg amex. In the early 1960s, pioneering studies by Jensen and colleagues suggested the presence of intracellular receptors for estrogens in target tissues. This was the first demonstration of receptors of the steroid/ thyroid superfamily and provided techniques to identify receptors for the other steroid hormones. In men, estrogens are produced by the testes, but extragonadal production by aromatization of circulating C19 steroids. Estrogens may be locally produced from androgens by the actions of aromatase or from estrogen conjugates by hydrolysis. Such local production of estrogens could play a causal or promotional role in the development of certain diseases, such as breast cancer, because mammary tumors contain both aromatase and hydrolytic enzymes. The placenta uses fetal dehydroepiandrosterone and its 16-hydroxyl derivative to produce large amounts of estrone and estriol. Physiological Actions Developmental Actions Estrogens are largely responsible for pubertal changes in girls and secondary sexual characteristics. Estrogens cause growth and development of the vagina, uterus, and fallopian tubes and contribute to breast enlargement. They also contribute to molding the body contours, shaping the skeleton, and causing the pubertal growth spurt of the long bones and epiphyseal closure. Growth of axillary and pubic hair, pigmentation of the genital region, and the regional pigmentation of the nipples and areolae that occur after the first trimester of pregnancy are also estrogenic actions. Androgens may also play a secondary role in female sexual development (Chapter 45). In boys, estrogen deficiency diminishes the pubertal growth spurt and delays cholesterol (the precursors of all steroids) transport into the mitochondria of cells, where androgen precursors are produced. Notably, theca cells of the ovary contain a form of 17-hydroxysteroid dehydrogenase (type I) that favors the production of testosterone and estradiol from androstenedione and estrone, respectively. All three of these estrogens are excreted in the urine along with their glucuronide and sulfate conjugates. Estrogen deficiency in men leads to elevated gonadotropins, macroorchidism, and increased testosterone levels and also may affect carbohydrate and lipid metabolism and fertility in some individuals (Grumbach and Auchus, 1999). At puberty the pulse generator is activated and establishes cyclic profiles of pituitary and ovarian hormones. The hypothalamic pulse generator located in the arcuate nucleus of the hypothalamus functions as a neuronal "clock" that fires at regular hourly intervals (A). This characteristic pattern of hormone secretions results from complex positive- and negative-feedback mechanisms (Hotchkiss and Knobil, 1994). At midcycle, serum estradiol rises above a threshold level of 150200 pg/mL for about 36 h. Changes in the ovarian follicle (top) and endometrium (bottom) also are illustrated schematically. Characteristic profiles are illustrated schematically for the follicular phase (day 9, inset on left) and luteal phase (day 17, inset on right). Both the frequency (number of pulses per hour) and amplitude (extent of change of hormone release) of pulses vary throughout the cycle. The midcycle surge in gonadotropins stimulates follicular rupture and ovulation within 12 days. In the absence of pregnancy, the corpus luteum ceases to function, steroid levels drop, and menstruation occurs. When steroid levels drop, the pulse generator reverts to a firing pattern characteristic of the follicular phase, the entire system then resets, and a new ovarian cycle occurs. In the luteal (or secretory) phase of the cycle, elevated progesterone limits the proliferative effect of estrogens on the endometrium by stimulating differentiation. Major effects include stimulation of epithelial secretions important for implantation of the blastocyst and the characteristic growth of the endometrial blood vessels seen at this time. Progesterone is thus important in preparation for implantation and for the changes that take place in the uterus at the implantation site. There is a narrow "window of implantation," spanning days 1924 of the endometrial cycle, when the epithelial cells of the endometrium are receptive to blastocyst implantation. Later, the placenta becomes the major site of estrogen and progesterone synthesis. Estrogens and progesterone have important effects on the fallopian tube, myometrium, and cervix. In the fallopian tube, estrogens stimulate proliferation and differentiation, whereas progesterone inhibits these processes. Also, estrogens increase and progesterone decreases tubal muscular contractility, which affects transit time of the ovum to the uterus. Estrogens increase the amount of cervical mucus and its water content to facilitate sperm penetration of the cervix, whereas progesterone generally has opposite effects. Estrogens favor rhythmic contractions of the uterine myometrium, and progesterone diminishes contractions. These effects are physiologically important and may also play a role in the action of some contraceptives. Estrogens affect many tissues and have many metabolic actions in humans and animals. The effects of estrogens on selected aspects of mineral, lipid, carbohydrate, and protein metabolism are particularly important for understanding their pharmacological actions. Bone is continuously remodeled at sites called bone-remodeling units by the resorptive action of osteoclasts and the bone-forming action of osteoblasts (Chapter 48). Estrogens directly regulate osteoblasts and increase osteocyte survival by inhibiting apoptosis (Kousteni et al. However, a major effect of estrogens is to decrease the number and activity of osteoclasts.