General Information about Lisinopril
If left untreated, hypertension can lead to severe well being problems, including heart illness, kidney disease, and stroke. This is why it could be very important monitor and manage blood strain levels via way of life changes and, if essential, medication similar to Lisinopril.
In conclusion, Lisinopril is an effective medication for treating hypertension and has been shown to significantly decrease the chance of heart illness and stroke. However, it should not be seen as an alternative alternative to a healthy lifestyle. A balanced food plan, common train, and stress administration strategies also wants to be incorporated in the management of high blood pressure. Remember, prevention is always higher than remedy, and early detection and treatment of hypertension can save lives.
The medicine comes in pill kind and is typically taken as quickly as a day, with or without food. The dosage may vary depending on the individual’s age, medical historical past, and response to treatment. It is necessary to comply with the prescribed dosage and to not stop taking the medication without consulting a physician, as abruptly stopping may cause a sudden increase in blood pressure.
Hypertension is a condition by which the force of blood towards the partitions of the arteries is constantly too high, placing a pressure on the heart and increasing the chance of coronary heart assault or stroke. It is estimated that over 1 billion folks worldwide have hypertension, making it some of the widespread persistent circumstances. Despite its prevalence, many people are unaware that they've hypertension, as it often presents with no symptoms. This is why it's often referred to as the “silent killer”.
Lisinopril is generally thought-about protected for use in most individuals, but there are some precautions to hold in mind. Individuals with a history of angioedema (swelling of the face, lips, tongue, or throat) mustn't take Lisinopril. It is also not beneficial for pregnant girls, as it might hurt the fetus. Therefore, it is essential to inform your doctor of any medical situations or drugs you take earlier than beginning Lisinopril.
Apart from its main use for hypertension, Lisinopril has additionally been discovered to be helpful in other conditions such as heart failure, diabetic kidney disease, and prevention of heart assaults in patients with a history of cardiovascular disease. This is why it's not unusual for medical doctors to prescribe Lisinopril to sufferers with these situations.
Lisinopril has been proven to effectively decrease blood stress, with research exhibiting that it might possibly cut back blood pressure by a median of 11/6 mm Hg. This discount in blood pressure not solely decreases the risk of coronary heart attack and stroke but also reduces the pressure on the guts, making it easier for it to pump blood around the physique.
Lisinopril works by inhibiting the exercise of the enzyme ACE, which is answerable for the manufacturing of a hormone known as angiotensin II. This hormone causes blood vessels to slender and constriction of blood circulate, resulting in increased blood stress. By blocking the production of angiotensin II, Lisinopril helps blood vessels relax and widen, allowing blood to move more simply and reducing blood stress.
Lisinopril is a drugs generally prescribed for the treatment of hypertension or hypertension in adults and children over the age of 6. It is part of a category of drugs generally recognized as angiotensin-converting enzyme (ACE) inhibitors, which work by relaxing blood vessels, allowing blood to circulate extra easily and lowering blood strain.
As with any medicine, Lisinopril may trigger unwanted effects in some individuals. The most typical unwanted effects embody a dry cough, dizziness, headache, and fatigue. In rare cases, more critical unwanted effects similar to severe allergic reactions, kidney problems, and liver issues might occur. It is essential to hunt medical consideration if any of those signs occur.
The molecular pathway for this synchronous segmentation has been termed the segmentation clock blood pressure medication online 5 mg lisinopril order otc. As new cells enter the paraxial mesoderm caudally, they begin phases of upregulation of the cycling genes, followed by downregulation of these genes. During each cycle, the most cranial presomitic mesoblast will segment and undergo mesenchyme to epithelial transformation to form the next somite. Experimental evidence (from chick embryos) shows that newly formed paraxial mesoblast cells undergo 12 such cycles before they finally form a somite (Pourquié and Kusumi 2001). Thus, from ingression through the primitive streak to segmentation into a somite takes approximately 18 hours. As the somite number varies between vertebrate species, it is likely that the rate of somite formation also varies and may be longer in human embryos. For an overview of vertebrate segmentation and its clinical implications, see Pourquié (2011). Processes from the somite cells pass through this basal lamina to contact the basal laminae of the neural tube and notochord. The compacted cells undergo a mesenchymal/epithelial transformation, resulting in an epithelial sphere of cells that surrounds free somitocoele cells. Shortly after the somite boundaries have been defined, there is a region-specific epithelial/mesenchymal transition of the ventral and ventromedial walls of the somite to form the mesenchymal sclerotome. As the embryo enlarges, the sclerotomal populations on each side become contiguous with the notochord and the neural tube. The rest of the dorsal lateral somitic epithelium remains as the epithelial plate of the somite, also termed the dermomyotome, a proliferative epithelium that will give rise to (nearly) all the striated muscles of the body. Segmentation of the paraxial mesoblast, mesenchymal/epithelial transformation to form epithelial somites and the resultant somite developmental processes (epithelial/mesenchymal transformation to form the sclerotome) all occur in a craniocaudal progression caudal to the otic vesicle from stage 9. The Golgi apparatus, actin and -actinin are all located in the apical region of the epithelial somite cells. The cells are joined by tight junctions (a variety of cell adhesion molecule has been demonstrated in epithelial somites). The cranial somites are at the upper border and the more caudal somites are at the lower border. The more cranially placed somites (at the lower right of the figure) are further developed than those caudally placed (at the upper left of the figure). The stages in somite development are given on the left of the figure; more detailed information is given on the right. BC, Diagrams of transverse (B) and longitudinal (C) sections through the somites; the plane in C is indicated by the dotted line in B. BC, Diagrams of transverse (B) and longitudinal (C) sections through the developing sclerotome; the plane in C is indicated by the dotted line in B. B, Longitudinal section through the dotted line indicated in A, showing the sclerotomal subdivisions. Hypaxial dermomyotome cells de-epithelialize from the ventrolateral edge and migrate into the limb bud. D, the local dermis is formed later by superficial de-epithelialization of dermomyotome cells. Each vertebra is formed from the cranial half of one bilateral pair of sclerotomes and the caudal half of the next pair of sclerotomes. The central sclerotome remains close to the dermomyotome; it will give rise to the pedicles and ventral parts of the neural arches, and the proximal ribs. The ventral sclerotomal cells, which were always laterally abutting the notochord, proliferate to form an axial cell population within the extracellular matrix of the perinotochordal space, now termed the perinotochordal sheath. The dorsal sclerotomal cells develop relatively late; they invade the space between the surface ectoderm and growing neural tube, and form the dorsal part of the neural arches. The lateral sclerotomal cells give rise to distal ribs and endothelial cells of blood vessels. Sclerotomal cells also give rise to the meninges surrounding the spinal cord, local tendons and ligaments. The somitocoele cells, which remain mesenchymal throughout somite formation, give rise to the vertebral joints, intervertebral discs and the proximal ribs (Christ et al 2004). Proliferation at the dorsomedial edge produces cells that elongate from the cranial to the caudal edge of the dermomyotome beneath its apical surface as they move laterally. Cells similarly proliferate from the cranial and caudal edges of the dermomyotome and these cells also elongate across it. The cells that are produced from these three edges are termed the epaxial myotome, and will give rise to skeletal muscle dorsal to the vertebrae, i. At limb levels, cells de-epithelialize and migrate from the ventrolateral edges of the dermomyotome into the limb bud. Cells produced from this portion of the occipital somites migrate anteriorly to give rise to the intrinsic muscles of the tongue. At interlimb levels, the hypaxial myotome will give rise to intercostal and abdominal muscles, and extend from the ventrolateral edge of the epithelial Development of sclerotomes dermomyotome into the body wall as development proceeds (Scaal and Christ 2004). It was thought that the somite gave rise to segmental portions of the dermis of the skin, as well as bone and muscle. However, it is now clear that the somitic contribution to the skin from the epithelial plate is limited to de-epithelialization of dermomyotomal cells over the epaxial muscles alone, which is a much smaller distribution than the segmental portion of skin usually implied by the term dermatome. The concept that an embryological dermatome, derived from the somite, produces all of the dermis of the skin is therefore outdated.
The multiple bones of the facial skeleton have diverse embryonic origins; the most significant in ageing are the odontogenic bones (maxilla and mandible) blood pressure medication beginning with d order 2.5 mg lisinopril overnight delivery. With the exception of the ear, all the cavities are located on the front of the face and their presence contributes to ageing of the mid-cheek. Musculoskeletal movement in the face is initiated only from the temporomandibular joint; the two major skeletal masticatory muscles (temporalis and masseter) are located beneath the deep fascia of the lateral face. The soft tissues overlying the lower third of the face are significantly impacted by this skeletal movement, as well as by the extensive movement of the subjacent neck. Active movement, a unique feature of facial anatomy, arises on the anterior face, primarily in relation to the orbital and oral cavities, as a result of the contraction of the sphincter muscles embedded in the soft tissues overlying the cavities. Movement around the orbit is modified by the forehead and glabellar musculature and by the orbital part of orbicularis oculi. The lip elevator and depressor muscles add to the lip movement around the oral sphincter. Movement on the lateral face is passive only, secondary to major tissue displacements extending from the anterior face, or to movement of the underlying mandible or neck. These muscles are intimately attached to the overlying soft tissues and skin, which they are programmed to move, and have minimal attachment to the underlying skeleton. A discontinuous glide plane layer beneath the muscle layer consists of spaces that allow movement of the overlying soft tissues. The soft tissues of the face are stabilized in position by an extensive fibrous support system that is unique to the facial structure (Furnas 1989, Stuzin et al 1992). The system takes its fixation from attachment to the underlying skeleton and provides strong direct support to the dermis via its layered arrangement. Overlying the cavities, the support system is necessarily modified by the absence of bone for ligamentous fixation, which means that support over the orbital and oral cavities is indirect. The support of the specialized, very mobile, soft tissues that form the eyelids over the orbital cavity and the part of the cheek that overlies the extensive vestibule of the oral cavity, together with the soft tissue apertures forming the lid margins and the lips, is therefore structurally compromised. Bony rims provide the skeletal base for this indirect ligamentous attachment around the bony cavities. Further adaptations of the fibrous support system are necessary over the oral cavity because here the bony rim is not fixed and continuous, as it is in the orbital rim, but enlarges with jaw movement. The combination of soft tissue movement over the orbital and oral cavities, along with the necessary reduction of ligamentous support to allow this movement, is the basis for the ageing of the soft tissue around the eye and around the mouth. Overview of facial ageing the general pattern with ageing is a progressive loss of facial volume with increasing laxity and possibly expansion of the outer layers with descent. The smooth, taut surface of a full and uniformly rounded youthful face deteriorates with ageing to form a series of individual segments that are separated by surface grooves located where internal ligaments attach to the dermis, and that progress to form skin creases or wrinkles as the dermis weakens (Mendelson and Jacobson 2008). Changes in one structure will have an impact on the others and, in more advanced ageing, simultaneous changes in more than one component will produce a cumulative effect. The only certain primary change is a loss of anterior volume of the maxilla that is associated with the eruption of the secondary dentition. The superficial muscles are in the middle layer (layer three), although muscle is not present in all areas of the face. Functionally, this layer is related to the skin, via the connections of the retinacula cutis in the subcutaneous layer, rather than to the deeper structures. The ligaments take origin from the deep fascia and form septa-like boundaries in the temple. Key: a, zygomatic ligament; b, uppermost masseteric ligament; c, upper key masseteric ligament; d, lower key masseteric ligament; e, mandibular ligament. From above, these structures are: temporalis fascia; arch of zygoma; masseter (largely overlain by the parotid and masseteric fasciae). The prezygomatic space overlies the body of the zygoma, between the orbicularis retaining ligament around the orbit above and the zygomatic ligaments above the oral cavity. A series of premasseteric spaces overlie masseter, in the interval between the concave anterior border of the parotid gland (including its accessory lobe) and the line of masseteric ligaments. These spaces allow gliding movement of the composite soft tissues associated with the oral cavity and opening the jaw. It covers the large area overlying the vestibule of the oral cavity and its support is limited largely to its superolateral corner, where it is provided by the zygomatic ligament. It overlies the masseteric fascia above the mandibular rim, and prevents soft tissue drag from movement of the mouth that would restrict opening of the jaw. However, when there is weakness of the lower masseteric ligaments (normally holding platysma in close relation to the masseteric fascia), the buccal fat pad becomes more mobile, and it may descend into a more anterior location towards the corner of the mouth, adding to fullness of the labiomandibular fold. The dimensions of the orbital aperture increase slightly but are significant in periorbital ageing. Recession of the inferolateral rim (by more than 10%) causes the greatest alteration of orbital shape. The changes exhibit sexual dimorphism in that they are generally seen at a younger age in women (by middle age) compared to men. Thus, a small increase of transverse orbital width and aperture area happens earlier in women, and superomedial recession occurs later and to a greater extent in men (Kahn and Shaw 2008). Soft tissue laxity of the lower face accompanies the reduction in size of the mandible. By middle age, there is a considerable reduction of the mandibular angle with shortening of the length of the mandibular body and its height; shortening of the height of the ramus occurs later (Pessa et al 2008, Shaw et al 2010). It is now known that the facial skeleton is not static and changes significantly with age. The skeletal origin of the ligaments continues from the anterior end of the superior temporal line, down the lateral orbital rim to the body of the zygoma, and down the anterior border of masseter to the mandibular ligament.
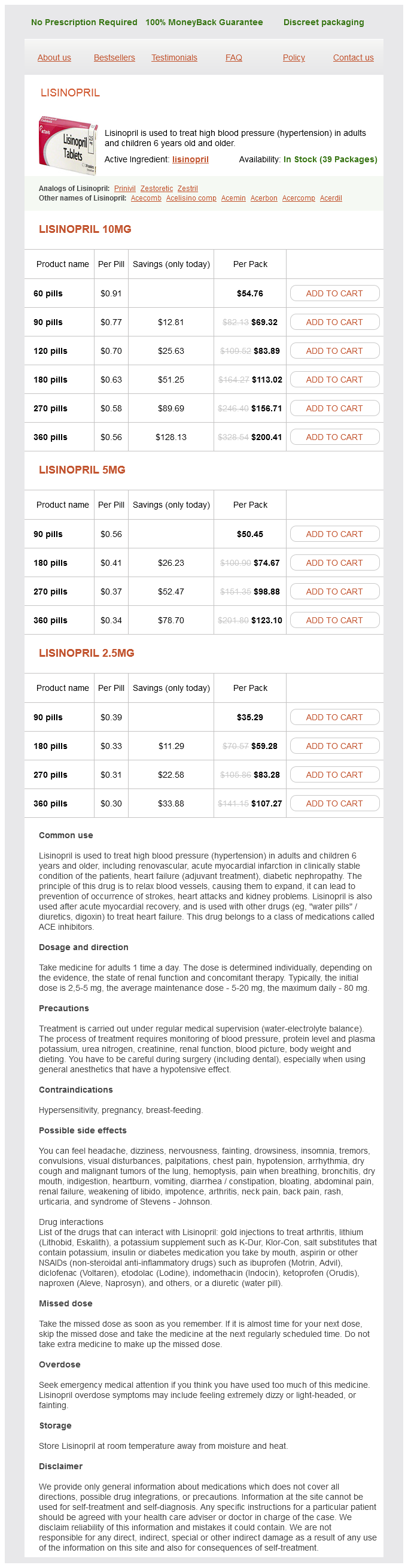
Lisinopril Dosage and Price
Lisinopril 10mg
- 60 pills - $54.76
- 90 pills - $69.32
- 120 pills - $83.89
- 180 pills - $113.02
- 270 pills - $156.71
- 360 pills - $200.41
Lisinopril 5mg
- 90 pills - $50.45
- 180 pills - $74.67
- 270 pills - $98.88
- 360 pills - $123.10
Lisinopril 2.5mg
- 90 pills - $35.29
- 180 pills - $59.28
- 270 pills - $83.28
- 360 pills - $107.27
Posteriorly pulse pressure measurement order generic lisinopril online, the surface is rough ened where it articulates with the perpendicular plate of the palatine bone. This surface is traversed by a groove that descends forwards from the midposterior border, and is converted into a greater palatine canal by the perpendicular plate. Anterior to the hiatus, a deep nasolacrimal groove, continuous above with the lacrimal groove, makes up about twothirds of the circumference of the nasolacrimal canal. The rest is contributed by the descending part of the lacrimal bone and the lac rimal process of the inferior nasal concha. More anteriorly, an oblique conchal crest articulates with the inferior nasal concha. The concavity below it is part of the inferior meatus, while the surface above it is part of the atrium of the middle meatus. Zygomatic process Anterior, infratemporal and orbital surfaces of the maxilla converge at a pyramidal projection, the zygomatic process. Anteriorly, the process merges into the facial surface of the body of the maxilla. Inferi orly, a bony arched ridge, the zygomaticoalveolar ridge or jugal crest, separates the facial (anterior) and infratemporal surfaces. A small, palpable tubercle at the junction of the crest and orbital surface is a guide to the lacrimal sac. The smooth area anterior to the lacrimal crest merges below with the anterior surface of the body of the maxilla. Parts of orbicularis oculi and levator labii superioris alaeque nasi are attached here. Behind the crest, a vertical groove combines with a groove on the lacrimal bone to complete the lacrimal fossa. A rough subapical area articulates with the ethmoid, and closes anterior ethmoidal air cells. Below this, an oblique ethmoidal crest articulates posteriorly with the middle nasal concha, and anteriorly underlies the agger nasi, a ridge anterior to the concha on the lateral nasal wall. Its anterior border articulates with the nasal bone and its posterior border articulates with the lac rimal bone. Alveolar process the alveolar process is thick and arched, wide behind, and socketed for the roots of the upper teeth. The socket for the canine is deepest, the sockets for the molars are widest and subdivided into three by septa, those for the incisors and second premolar are single, and that for the first premolar is usually double. Buccinator is attached to the external alveolar aspect as far forwards as the first molar. Occasionally, a variably prominent maxillary torus is present in the midline of the palate. Frontal process the frontal process projects posterosuperiorly between the nasal and lacrimal bones. Its lateral surface is divided by a vertical anterior 485 cHapTeR B 30 Face and scalp Palatine process the palatine process, thick and horizontal, projects medially from the lowest part of the medial aspect of the maxilla. It forms a large part of the nasal floor and hard palate, and is much thicker in front. Its infer ior surface is concave and uneven, and with its contralateral fellow it forms the anterior threequarters of the osseous (hard) palate. The palatine process displays numerous vascular foramina and depressions for palatine glands and, posterolaterally, two grooves that transmit the greater palatine vessels and nerves. The infundibular incisive fossa is placed between the two maxillae, behind the incisor teeth. The median intermaxillary palatal suture runs posterior to the fossa, and although a little uneven, is usually relatively flat on its oral aspect. Its bony margins are sometimes raised into a prominent longitudinal palatine torus. Two lateral incisive canals, each ascending into its half of the nasal cavity, open in the incisive fossa; they transmit the terminations of the greater palatine artery and nasopalatine nerve. Two additional median openings, anterior and posterior incisive foramina, are occa sionally present; they transmit the nasopalatine nerves, the left usually passing through the anterior, and the right through the posterior foramen. On the inferior palatine surface, a fine groove, sometimes termed the incisive suture, and prominent in young skulls, may be observed in adults. It extends anterolaterally from the incisive fossa to the interval between the lateral incisor and canine teeth. The superior surface of the palatine process is smooth, is concave transversely, and forms most of the nasal floor. The medial border, thicker in front, is raised into a nasal crest that, with its contralateral fellow, forms a groove for the vomer. The front of this ridge rises higher as an incisor crest, prolonged forwards into a sharp process that, with its fellow, forms an anterior nasal spine. The posterior border is serrated for articulation with the horizontal plate of the palatine bone. The palatine surface forms the posterior quarter of the bony palate with its contralateral fellow. The posterior border is thin and concave; the expanded tendon of tensor veli palatini is attached to it and to its adjacent surface behind the palatine crest. Medially, with its contralateral fellow, the posterior border forms a median posterior nasal spine to which the uvular muscle is attached. The anterior border is serrated and articulates with the palatine process of the maxilla. The lateral border is continu ous with the perpendicular plate of the palatine bone and is marked by a greater palatine groove. The medial border is thick and serrated, and articulates with its contralateral fellow in the midline, forming the posterior part of the nasal crest which articulates with the posterior part of the lower edge of the vomer.