General Information about Isoniazid
Isoniazid is a first-line antibiotic drug used within the remedy of tuberculosis. It was first developed in 1912 however was not broadly used till the Fifties. Isoniazid is a half of the class of medicines referred to as antimycobacterials, which are drugs used specifically to deal with TB. It is available in varied types, including tablets, injections, and syrups.
More critical unwanted effects can also occur, though they're much less common. These might embody liver injury and allergic reactions. Signs of liver injury might embody yellowing of the skin or eyes, dark urine, abdomen ache, or uncommon tiredness. Individuals ought to search medical attention immediately if these signs occur. Allergic reactions to Isoniazid might present with difficulty breathing, swelling of the face, lips, tongue, or throat.
Isoniazid is primarily used for the therapy of tuberculosis, which is a highly infectious bacterial disease that primarily impacts the lungs but can even have an result on different components of the body. It is commonly utilized in mixture with different TB medicines corresponding to rifampin, ethambutol, and pyrazinamide to realize maximum effectiveness.
Precautions
Isoniazid, also referred to as INH, is an antibiotic medication generally used for treating or preventing tuberculosis (TB) infection. This drug has been in use for over 50 years and has been a pivotal element in the remedy of TB. In this text, we'll discover what Isoniazid is, the way it works, its uses, unwanted effects, and precautions.
Isoniazid works by killing the micro organism that cause TB, often recognized as Mycobacterium tuberculosis. It does this by inhibiting a selected bacterial enzyme known as enoyl-acyl service protein reductase, which is crucial for the bacteria's survival and replication. By blocking this enzyme, the micro organism are unable to provide certain important proteins, ensuing in their dying.
Side Effects of Isoniazid
In conclusion, Isoniazid is a crucial medicine within the remedy and prevention of tuberculosis. Its effectiveness and relatively low price have made it a vital drug for both growing and developed international locations within the struggle towards TB. However, it is essential to consult with a well being care provider before taking this medicine to ensure its safe and efficient use. Along with proper diagnosis and administration, Isoniazid can play a significant function in eradicating TB and saving lives.
How does it work?
Certain precautions should be taken before beginning Isoniazid treatment. Individuals with liver illness, a historical past of alcoholism, or who're taking other medications which will have an result on the liver ought to inform their physician before taking Isoniazid. It can be essential to inform the doctor in case you have diabetes, kidney disease, or HIV infection, as these situations could affect the selection of therapy or dosage.
What is Isoniazid?
Uses of Isoniazid
Furthermore, Isoniazid is also used for preventive therapy in individuals who have been uncovered to TB but haven't but developed the an infection. This is commonly the case for people who repeatedly are available contact with TB sufferers, such as health care employees. It can be utilized in combination with other medication for the remedy of latent TB an infection (LTBI), which means that the micro organism are current within the physique however not currently active.
Furthermore, people who are pregnant or breastfeeding should discuss with their doctor about the potential dangers and benefits of taking Isoniazid. While this medication is generally considered secure, warning must be exercised during being pregnant or breastfeeding.
Like another medication, Isoniazid may cause some unwanted effects in some people. The commonest side effects embody nausea, vomiting, and lack of appetite, which normally subside after a couple of weeks of therapy. Other side effects could embody rash, fever, headache, changes in vision, and numbness or tingling in the hands and toes. These unwanted facet effects should be reported to a well being care provider if they turn into bothersome or extreme.
However treatment upper respiratory infection isoniazid 300 mg purchase without prescription, the patient can learn to acknowledge the deficit in his communication and to compensate for it. The patient and his relatives can be directed in ways to communicate to the injured and in which situations they should stop the excessive talking. In reflexive crying and laughing, we can attempt to inquire of the patient, when he is relaxed, how he wishes to deal with the issue. Effects of Brain Injury on Emotional Reactions 93 Patients suffering from severe reflex crying often wish that no attention be paid to them. Those suffering from milder symptoms may wish for a sign of empathy, such as a light touch. Some can learn to control the symptoms by moving their attention or line of vision elsewhere for a moment. Therapist and patient together can think of ways for the patient to communicate his or her symptoms. If the patient suffers from reflexive laughter, the people around him should know not to laugh with him. If emotional expression has subdued, it is important for relatives to learn how not to take it personally. We can attempt to stimulate emotional reactions with objects and things the patient has liked in the past (such as, photographs, movies, places, experiences, etc. In instances of over sensitive reactions, it is important to stay calm and empathetic, without joining the emotional outburst and making it stronger. When it has been clearly established that lability is an organic, not a psychological, reaction to illness, it is good to make this obvious to relatives. Specific analysis of the symptom situation can clarify both the provoking and the relieving factors (for example, exhaustion, pain, hunger, etc. At times it is good to avoid situations in which reactions are heightened, especially at the beginning. It can be investigated as to whether shifting attention, moving away from the situation, or external hints have any effect. If lability is permanent and disturbing, some traditional methods of cognitive therapy can be used if they help with the symptom or with getting used to it. In anger and fits of rage, psychoeducation should also be used, along with guidance and investigating what the provoking actors are. It is essential to avoid overstimulation, learn strategies of selfcontrol, and, if needed, create a safe environment. It is important to explain peacefully to an easily angered person what is in fact is happening, as many outbursts are due to confusion or overloading. Brain damage can weaken the skill to adapt to rapidly changing situations, and many patients do not like "surprises. The methods range from external to internal control, supporting personal acceptance of symptoms, and psychoeducation to specific psychotherapeutic techniques. In some cases, the awakening or strengthening of emotional expression is justified; in others it is not. Greenberg & Paivio (1997), for example, does not recommend the reinforcement of emotions in patients with inadequate regulation skills or clearly impaired cognitive abilities, nor those depicting psychotic behavior or suffering from severe borderline personality disorders. Additionally, it is important to keep in consideration that emotions can get "stuck" easily in organic emotional problems. After brain injury, the patient often has to redefine his sense of "self," as previously established modes of behavior do not necessarily function any longer. Individuals will strive to maintain the sense of continuity of self, although they might notice that their own actions and ways of thinking are not quite as they used to be. There are ways to support the integration process, such as narrative methods and suggesting the creation of self portraits, by helping to interpret and name occurrences and experiences, and by encouraging the patient to join peer-support groups. Not all patients require formal therapy, but most need at least some guidance and aid (Judd, 9 (1999)). Effects of Brain Injury on Emotional Reactions 95 A Case Description-Emotional Monitoring, Memory, and the Self Following is a description of a neuropsychotherapeutic rehabilitation case, in which psychological rehabilitation has been combined with psychotherapy. She had severe symptoms in the frontal lobe, which made controlling emotions and behavior difficult and interfered with memory and concentration. In a neuropsychological test carried out at the hospital, the following findings were made typical for frontal region damages: slight difficulties in executive functions, a tendency to repeat or mix up memories, mild problems with finding words, problems with inhibiting stimuli, slowness, a tendency to make mistakes, and a slightly narrow auditory attention span. The estimate was, however, that the entire magnitude of the symptoms might not be revealed in a structured testing situation. Doing her homework was taking up more time than in the past, and in exams she ran out of time. The Course of the Rehabilitation Process: Challenges in Behavior and Everyday Life Caused by Damage to the Frontal Lobe In the beginning, it became apparent that studying for two degrees simultaneously was too much. Her relatives explained how she studied actively but did not succeed as she had in the past. She was studying for a profession she had dreamed of since childhood-she felt as if she had to succeed. To the outsider, she gave an impression of herself as diligent and energetic, and she had not cried for years. At times, she would become disturbed by getting her thoughts mixed up and experiencing déjà vu.
Specific disease entities require different approaches medications ordered po are buy 300 mg isoniazid with visa, as for cognitive training methods and/or psychotherapeutic techniques. However, as described previously in this chapter, emotional experiences with good working alliance should always be targeted as a general element in the treatment procedure. The basic knowledge of neuroscience research concerning the different diseases is abundant and can be a challenge to a neuropsychologist working with different types of etiologies. Localization aspects may have a unifying value despite the mechanism producing the disorder. Borod (2000) has described emotional changes in different disease entities as well as the domains of emotional experiences varying from perceptual sensations to emotional reactions. It is possible to differentiate between emotions themselves and the domain or element of a particular emotion, which is lacking. In clinical practice, there are patients who have "lost the ability to feel" or "experience" a certain emotion, even though the perceptions are accurate and the reaction, such as crying, may seem to indicate emotional processing. Coping responses, such as avoidance, worry, and rumination, are ways in which patients aim to reduce this threat. Threat is suggested to impact processes that allow integration of traumarelated representations in to prior, enduring representations of self, others, and the world. In uncovering underlying traumatic meanings, personal values and expectations need to be considered. Neuropsychotherapeutic Approaches in the Rehabilitation Context 15 the Innuences of Personality Predispositions and the Basis for Healthy Attachment in the Course of Development In real life therapy situations, the therapist will face an immense amount of patients with different life histories and personality types. There is no single guideline as to how we should define people, as far as the concept of personality is concerned. Cognitive theory considers personality to be grounded in the coordinated operation of complex systems that have been selected or adapted to insure biological survival (Alford & Beck, 1997). Further cognitive definition of personality includes individual schematic processes, which theoretically determine the operation of major systems of psychological analyses. Young, Klasko, and Weishaar (2003) have built up a schema model, and Greenberg & Paivio (1997) have created a conceptual model from a constructivist cognitive framework. Schemas have also been called core beliefs, which guide our cognitive, emotional, and behavioral perceptions of the world and reactions to situations from moment to moment. Negative beliefs and biased views of the world make us vulnerable to depression (Clark, Beck, & Alford, 1999), and over- or underdeveloped belief systems may distinguish between anxiety and depressive symptoms. Cognitive distortions like catastrophizing, personalization, magnification and minimization, selective abstraction, arbitrary inference, and overgeneralization are typically seen in psychiatric states of overload of emotional reactions (Freeman, Pretzer, Fleming, & Simon, 1990). If a patient is inclined to think of himself in a distorted way in case of difficulties. How the autobiographical history can explain and give background to this kind of development may also be viewed by attachment models. According to Allen (2001), attachment is the foundation for distress regulation in clinical practice. Our task is one of pattern recognition and identifying recurring themes in interactions. The process of attachment is the basis for emotional development from the first months of life through the growing years. The attachment types and their influence in adulthood can be classified as follows: 1. Avoidant attachment ° avoiding, matter-of-fact, polite, good performing/achieving behavior 3. The Interpersonal Process, Its Ruptures, and Building a Good Working Alliance Neuropsychological rehabilitation, or cognitive rehabilitation, as it has been also called, has traditionally placed less importance on the therapeutic relationship, until increasing interest in the past years. The same trend seems to apply to cognitive behavioral therapies (Safran & Muran, 2000). Poor outcome shows a negative interpersonal process independent of the therapeutic modality. The patient and the therapist Neuropsychotherapeutic Approaches in the Rehabilitation Context 17 Mutual engagement and alliance is a dynamic process in which emotional contact with the patient is essential A good alliance is a prerequisite in all treatment situations. Safran and Muran (2000) find relational theory to be particularly useful for organization of insights and principles from other therapeutic traditions that are relevant to the topic of therapeutic impasses and resistance (Leahy, 2001). In this book, resistance is a separate chapter, and the interpersonal process is discussed in more detail in the chapter on therapeutic methods. The strength of alliance is dependent on the degree of agreement between patient and therapist about the tasks and goals of therapy and the quality of the relational bond between them. Interpersonal and relational perspectives provide more scope for more technical flexibility. When faced with resistance or noncompliance, the therapist should ally with it, not attempt to invalidate or undermine it. The relational process is always a dynamic moment-to-moment procedure, no matter how structured the therapist aims to be. According to Safran and Segal (1990), the theory process can be thought of as a series of events unfolding over time at three levels: 1. This understanding gives freedom to the therapist for a relaxed and flexible collaboration with the patient. The Nature of Neuropsychological Demcits and Knowledge of Specimc Methods of Cognitive Retraining Neuropsychotherapy should include cognitive training when it is a necessary goal. Neuropsychological disturbances are most likely best known to clinical neuropsychologists. Johnstone and Stonnington (2001) point out that, although significant strides have been made in the development of tests to assess brain function, there is still need to develop effective treatment interventions to improve specific neuropsychological impairments, and ultimately the lives of persons with brain dysfunction.
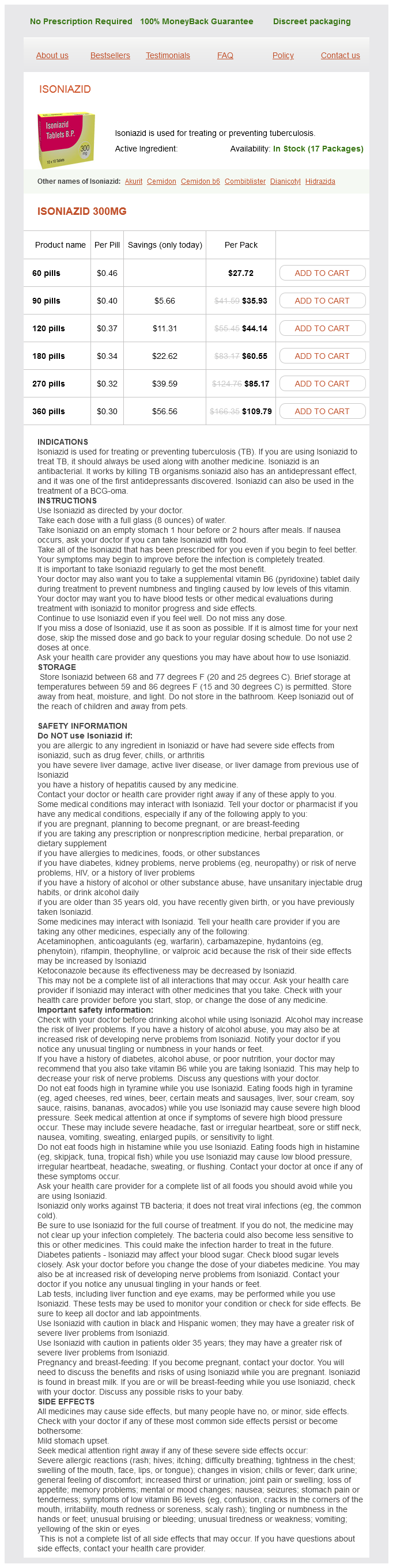
Isoniazid Dosage and Price
Isoniazid 300mg
- 60 pills - $27.72
- 90 pills - $35.93
- 120 pills - $44.14
- 180 pills - $60.55
- 270 pills - $85.17
- 360 pills - $109.79
A pre-hernial lipoma must be isolated from the spermatic cord medications you can give dogs buy cheap isoniazid 300 mg, ligated and sectioned at the deep inguinal ring. A different approach is required for treating sliding hernias, which are large hernias often of long duration. The hernia contains the hernia sac formed by the peritoneum, in addition to intraperitoneal and partly extraperitoneal organs that, accompanying the hernia sac, slips down. The bladder and the cecum can be found on the right and the pelvic colon on the left. Preoperative diagnosis may be difficult, as a sliding hernia is usually incidentally discovered during surgery. B: Finger detachment of the sper· matic cord from the posterior wall of the inguinal canal. Unwary isolation and opening of the hernia sac can increase the risk of inadvertent injury to the intestine or bladder. The best treatment is resection of the excess peritoneum of the sac, without removing the visceral adhesions. The serosa is closed with a continuous suture and the adherent herniated bowel is freed from adhesions to the parietal structures and reduced in to the abdominal cavity. The cord, put on two laces, is moved down, two Klemmer forceps grasp the extremity medial and lateral to the inferior edge of the external oblique fascia above the spermatic cord. Opening of the Tranavtmilalis Faacia the transversalis fascia is incised parallel to the inguinal ligament. The preperitoneal fat is pushed away from the transversalis fascia to move the peritoneum and the bladder, displaying the rectus abdom. In cases of direct inguinal hemia, the sac can be dissected after opening the fascia transversalis. In such cases, it is unnecessary to treat the peritoneal sac; instead, it is sufficient to remove the fat from the posterior aspect of the fascia transversalis and push it down deeply. The redundant and weakened part of the transversalis fascia is resected at the lower edge of the transverse and internal oblique muscles. The lower edge of the transversalis fascia almost always shows a marginal vein internally that should be tied or cauterized to avoid troublesome bleeding. B: Opening the transversalis fascia from the lateral margin af the deep inguinal ring to the pubic tubercle. This is a fundamental step in the Bassini operation, as it also permits exploration of the femoral region. A Farabeuf retractor holds the triple layer and the underlying structures superiorly, making it easy to place the first suture below the tubercle, the pubic periosteum and the inguinal ligament. Subsequent sutures include the triple layer superiorly, about 3 em from its lower edge, and staggered 1 em apart from each other to avoid involvement of the iliohypogastric nerve. The sutures are tied without excessive traction; the triple layer is simply apposed with the inguinal ligament; sutures tied too tightly can cause ischemia and cut the affected tissues. With the last stitch the deep inguinal ring is rebuilt, which must not be tied too tight, otherwise it will compress the cord vessels. The tip of the finger should be able to commit at this level and the axial mobility of the cord contents checked by traction using forceps after having tied the last suture. Therefore, among the changes later advanced was the more successful Shouldice technique proposed some 50 years ago. The principle is the same as that of the Bassini operation: the Shouldice technique diHers in that the triple layer is sewn to the inguinal ligament and the iliopubic tract with multiple continuous sutures instead of loop sutures. In this way, the tension on the repaired tissue is reduced, with less space between the tissues and the elimination of areas of weakness between stitches that may occur with the Bassini technique. The authors suggested using deep suture loops for parietal reconstruction, as Bassini had originally conceived of in his technique, wherein a suture is placed in the double layer of the transversalis fascia, corresponding precisely to the first and second suture lines of the Shouldice technique. This reconstruction of separate transversalis fascia is performed after passing all the sutures between the inguinal ligament and the triple layer before finally tying it In this way, the tension at the suture is reduced, starting at the deepest plana. This allows a stronger scar to form, ultimately producing a more physiologic and stronger reconstruction, with recurrence rates similar to the method devised by Shouldice. Today, tension-free hernia repair techniques have largely replaced these interventions: They are more easily learned, and mora quickly performed, with a very satisfactory postoperative course. The number af sutures varies from six to eight depending on the length af the inguinal canal. They should not be tied too tight so as to avoid ischemia and shearing through the affected tissue. Today, the choice of technique is orientated to "customized" repair on the basis of place, size, type of defect, patient age, and clinical condition. What remains is the wealth of knowledge, experience, and treatment methods such as the Bassini technique, one of the great achievements in the history of medical science. It typically requires a relaxing incision and careful dissection near the femoral vessels. It provides closure of the femoral, indirect and direct spaces, and, as such, can be used to repair any hernia defect that may occur in the groin. Femoral hernias account for 2% to 4% of groin hernias, are more common in women, and are more apt to present with strangulation and require emergency surgery. The postoperative morbidity and mortality increase significantly in patients undergoing emergent repair. This highlights the importance of repairing femoral hernias in an elective setting and suggests that watchful waiting is not a prudent strategy in patients with femoral hernias, even those who are asymptomatic. The Cooper ligament repair is rarely performed today, as it has been replaced by tension-free prosthetic mesh repairs. The well-known advantages of tension-free hernia repair have led to the development of various mesh techniques for femoral hernia repair. In addition, a laparoscopic approach provides an excellent repair of femoral hernias.