General Information about Geriforte Syrup
Not only does Geriforte Syrup have a optimistic impact on mental well-being, but it additionally helps to decelerate the degenerative modifications that happen within the physique over time. By accelerating cellular regeneration and restore, this natural supplement may help to fight the results of getting older, making it a well-liked selection among individuals looking to maintain their youth and vitality.
Geriforte Syrup is easy to devour, with a really helpful dose of 1 teaspoon twice every day. It can be protected for long-term use, with no unwanted facet effects reported. However, as with every herbal complement, it is always advisable to seek the guidance of with a healthcare skilled earlier than beginning any new supplement.
In conclusion, Geriforte Syrup is a robust and pure answer for individuals trying to relieve stress and promote overall well-being. With its potent adaptogenic and rejuvenating properties, it can assist to scale back stress-related diseases and promote healthy getting older. So, if you're on the lookout for a pure way to combat stress and feel extra energized, Geriforte Syrup could be the excellent supplement for you.
Another key ingredient in Geriforte Syrup is Amalaki or Indian Gooseberry, which is wealthy in antioxidants and highly effective immunomodulators. This superfruit is known for its rejuvenating results on the body, serving to to fight free radicals and promote wholesome mobile regeneration.
Geriforte Syrup also contains Licorice, a herb recognized for its anti-inflammatory properties, which helps to alleviate physical and psychological fatigue. It can additionally be a pure source of cortisol, a hormone that helps the physique in times of stress.
The major ingredient in Geriforte Syrup is the Indian Winter Cherry, also called Ashwagandha, a robust adaptogenic herb that has been used in Ayurvedic drugs for its restorative properties. Ashwagandha is thought for its capacity to help the physique adapt and deal with physical and mental stress, making it an ideal ingredient for a stress-relieving complement.
Geriforte Syrup is a pure natural complement that has been used for centuries to help fight stress and promote total well-being. Originating from the Himalayas, this potent formulation is produced from a mix of traditional Ayurvedic herbs, specifically designed to boost vitality and rejuvenation.
The Geriforte Syrup method also contains Guduchi, an adaptogenic herb that reinforces the physique's natural defenses towards stress and toxins. Guduchi is thought for its capability to reinforce vitality, enhance immune operate, and promote tissue repair.
Together, these ingredients work synergistically to help scale back stress, promote higher sleep, and improve general well-being. Geriforte Syrup has been scientifically confirmed to be effective in combating stress-related disorders, corresponding to anxiety and continual fatigue syndrome. It is also a preferred alternative among people trying to improve their psychological focus and focus.
The choice of pH and formulation components plays also a critical role in maintaining glass container (primary packaging) integrity and leaching of extractables from rubber stoppers herbals names buy geriforte syrup 100 caps amex. Alkaline pH could promote, for example, dissolution of silica from glass, resulting in pH changes of the formulation during long-term storage. Excipients for the prevention of protein degradation and aggregation of therapeutic antibodies seem to exert their effects via a number of different pathways. These include the following: 1) Binding of the excipient to the protein and stabilization of the native conformation. Examples of such direct proteinÎ¥xcipient interactions have been observed for, for example, polysulfates or cyclodectrins; 22. Potential solutions pH control, surface-active excipients, reduction of interfaces, especially water/air interfaces, minimization of mechanical and shear stress reduction of protein-interface interactions (especially at water/air interface), minimization of mechanical and shear stress, surface-active excipients, pH control Surface-active excipients, reduction of interfaces, especially water/air interfaces, minimization of mechanical and shear stress, control of proteinÎ¥xcipient interactions Surface presaturation, presence of surface-active excipients, optimization of protein concentration, pH pH control and optimization, buffers pH control and optimization, product purity (especially for cleavages due to proteases), inhibitors pH control and optimization pH control, buffers, low ionic strength Chelating agents, antioxidants, low pH, oxygen-free/reduced processing and packaging Low pH, chelating agents pH control, buffers Thiol scavenger. According to this mechanism, the protecting role of excipients such as poly(ethylene glycol), amino acids, polymers, polyols, sugars, or other substances with multiple hydroxyl groups, has been described; 3) Prevention of proteinΰrotein or proteinγurface interactions or increasing solubility of the aggregates. Many of the above-mentioned excipients [101] are able to increase protein stability and/or inhibit irreversible aggregation and thus maintain protein integrity. These effects can be explained by an increased difference in free energy between the native and the denatured states, stabilizing the native state by making it even more energetically favorable than any unfolded state. Stabilizing excipients acting as co-solvent increase the protein stability by inducing a preferential hydration of the protein. This effect reduces the frequency of proteinΰrotein interactions and limits their ability to initiate nucleation and therefore protein aggregation. However, other degradation pathways and stresses have then to be taken into account and addressed specifically. Because several degradation pathways are mediated by water, the removal of water strongly slows down the degradation kinetics. As a consequence, the shelf-life of freeze-dried products is longer compared to that of the corresponding liquid formulations [102]. However, to stabilize proteins in the solid form, various specific excipients are necessary to maintain protein conformation and with this the biological activity [103]. Cryoprotectants are used to protect biologics from freezing damage, whereas lyoprotectants are stabilizers used to prevent denaturation of proteins during freeze-drying and subsequent storage in the dried state. Lyoprotectants act as a substitute for water molecules (which are removed in the lyophilization process) by forming new hydrogen bonds with the excipient. The effectiveness of excipients in the solid state to stabilize protein structures depends on three main factors [104ͱ06]. Besides the formulation composition, the stability of freeze-dried products is also determined by the freeze-drying process, as has been described extensively elsewhere. Especially with the upcoming new molecule formats such as Tandab (tandem diabody) or BiTe, which are extremely potent molecules, the drug product is formulated at low protein concentrations (0. Therefore, strategies have to be developed to avoid protein loss due to protein adsorption. On the other side, subcutaneous application of antibodies requires the development of formulation with protein concentrations >200 mg ml-1 to reach the therapeutic dose. For such highly concentrated protein formulations, colloidal instability becomes a major issue, besides the chemical degradations also observed for lower protein concentration regimes [109]. Because of the fact that each protein molecule (and even mAbs) acts as a single individual with a large number of often underestimated specific properties, only general strategies for the development are available. The formulations of most biopharmaceuticals are therefore developed case by case taking the individual demands for clinical studies and marketing as well as the application route into account. However, technical expertise and technical characterization of large-scale unit operations and systems enable scale-up concepts that result in the reproducibility of key process parameters within a given range across the scales [110]. This means that the experiments at the laboratory scale are meaningful for the large-scale systems and that the optimal small-scale process can be transferred successfully to the final manufacturing scale. Treatments with antibodies also require multiple doses and/or long-term administrations, especially 640 22 Process Development and Manufacturing of Therapeutic Antibodies when targeted at tumor growth in cancerous diseases. Such proteins are therefore needed in large quantities, and consequently large manufacturing capacities are necessary for the annual market supply for therapeutic antibodies. Typically, scale-up attempts are carried out by using a fermenter with the same geometry to illustrate the physical conditions in production fermenters. During the passages, volumes are raised gradually to achieve the optimal seed density of the production fermenter. After the inoculum phase, cells are incubated in 1ͳ prefermenters with increasing volumes before inoculation in the production fermenter takes place. Depending on the fermenter volume and product, mammalian cell cultures are cultivated mostly in a fed-batch process for 1ͳ weeks before the secreted recombinant protein is purified from the supernatant. For the production in large-scale fermenter ranging from 2000 l (2 kl) to 25 000 l (25 kl), critical parameters for a successful transfer and operation are agitation and aeration of the cell culture. In addition to these parameters, nutrients, the used cell line, and concentration of inhibitors influence the growth and productivity of the cell culture. Nonoptimal agitation or aeration of the cell culture leads to the following: × inhomogeneous agitation of the gas-liquid phase; × physical damages of the cells; × formation of concentration gradients. Mass transfer of oxygen from the gas phase into the liquid phase is critical particularly for all aerobic processes because of the required oxygen for metabolic processes and low solubility of oxygen in the liquid. The mass transfer of oxygen is directly proportional to the mass transfer coefficient (kL A) which is dependent on the vessel geometry, dispersion, pressure, media composition, and sparger. Ordinarily, the sparger is located at the bottom of the vessel to allow efficient mass transfer of process air.
Dilemmas in critical care One of the most difficult questions relating to critical care is determining when the patient should continue to be offered support or whether treatment has become futile herbals companies generic 100 caps geriforte syrup. Regardless of an oncology diagnosis, the mortality from severe sepsis is high, a recent study in Europe suggesting a mortality as high as 40%. This information should be borne in mind in any discussion with the patient and family irrespective of a cancer diagnosis. For some patients with a guarded prognosis due to underlying disease, consideration must be given to the purpose and utility of critical care. Early experience of critically ill patients with cancer demonstrated poor outcomes and few survivors. To an extent this became a self-fulfilling prophecy, with patients either not being referred, or those that were referred often being severely unwell with little chance of recovery. The best method of improving patient outcome is early detection and treatment of sepsis on the ward prior to coming to a critical care environment. Survival in days according to the number of dysfunctional organs is shown out to 1 year. The emphasis for oncology patients, therefore, should be on early detection and intervention to prevent and treat clinical deterioration. This should include pathways to rapid identification of the deteriorating patient, early intervention for organ dysfunction, and the administration of broad-spectrum antibiotics to cover likely infective agents. It is key that all staff involved in the care of patients at risk of deterioration are familiar with the identification and initial treatment of this group of patients. The early involvement of critical care (outreach) teams will support the parent team looking after a patient, and may allow intervention on the ward to prevent further deterioration and facilitate escalation of care as appropriate. However, it is worth keeping in mind that mortality escalates sharply with an increasing number of failing organs. Despite this effort, after three days it was apparent that the patient was not responding to treatment and was continuing to deteriorate. After discussion with the family it was agreed that the emphasis of care should switch to symptom control. It is impossible to know if earlier treatment of the infection would have altered his clinical outcome; however, the limited available evidence does suggest that early identification and appropriate treatment of infection in the general clinical population may improve outcomes. Long term prognosis and quality of life following intensive care for life-threatening complications of haematological malignancy. The association of sepsis syndrome and organ dysfunction with mortality in emergency department patients with suspected infection. In 2012, approximately 186 400 new cases of cancer and 75 700 cancer deaths were expected in Canada,1 and 1 638 910 new cases of cancer and 577 190 cancer deaths were expected in the United States. There are significant differences in how cancer services are delivered and paid for in the two countries. In Canada, most health services, including cancer care, are paid for publicly with legal residents of Canada being entitled to receive medically necessary services without co-payment. When it comes to cancer care specifically, most Canadian provinces have elected to develop provincial agencies such as Cancer Care Ontario11 or the British Columbia Cancer Agency12 to organize and deliver cancer services. As a result, most Canadian provinces have a centralized approach to cancer services delivery, with networks of regional cancer centres and various affiliated institutions providing the vast majority of specialized services such as radiation and chemotherapy. These are composed of public programmes, such as Medicare (for individuals older than 65), Medicaid (for low-income families and individuals) and the Veterans Affairs Health Care System (for veterans), in addition to a wide variety of private insurance plans usually obtained as part of an employment package. There is also a substantial proportion of Americans younger than 65 who are uninsured; however, with the passage of the Patient Protection and Affordable Care Act in 2010, most Americans are expected to have access to health insurance either through publicly funded programmes, employer-sponsored plans, or by purchasing individual coverage through health insurance exchanges. Whilst this may provide patients with many providers to choose from, it can also result in care that is delivered across multiple settings and is often fragmented. At present, management of acute issues in oncology has focused on three aspects of care: use of preventative strategies, patient education and telephone support. Guidelines have been developed recommending appropriate antiemetics for prevention of chemotherapy and radiotherapy-induced nausea and vomiting,17 and prophylaxis for febrile neutropenia. Some centres have also developed formal chemotherapy teaching classes that provide patients and their caregivers with information regarding potential side effects and their management. However, less is known about the effectiveness of patient education with respect to their ability to self-manage side effects and this is an area of active research. In addition, most centres provide access to telephone advice for urgent care issues although fewer centres have the capacity to see patients in urgent care clinics or can provide advice outside of clinic hours. Furthermore, present telephone support tends to be reactive rather than proactive. For specific acute issues, such as febrile neutropenia, protocols for management of low-risk patients in the outpatient setting have been developed, although their rate of uptake is unknown. The goals of the programme are to improve quality of care and patient satisfaction while optimizing care efficiency. This is felt to lead to cost savings, with preliminary evaluations in the primary care setting showing encouraging results. Studies have found that a significant proportion of patients with end-stage cancer receive aggressive care at the end of life, defined as chemotherapy close to death, admissions to hospital and intensive care units within the last few weeks of life, and underuse of hospice services. This is further reinforced by recent studies, which have shown significant benefits of early palliative care and better end-of-life care on survival,26 quality of life27 and aggressiveness of care in patients with end-stage cancer. More recently, the Canadian Partnership Against Cancer, has undertaken pan-Canadian tracking of cancer quality that is reported in an annual report. The programme continues to grow and evolve, and is currently being used by approximately 10% of American oncology practices. Novel multifaceted models that promote patient engagement and a comprehensive approach to care are currently being developed and may change the way acute problems are managed in cancer patients in North America in the near future. Quality measurement has and continues to be a widely used tool in both countries to drive transformation of health care delivery to improve quality of care and foster fiscal sustainability. The Canadian Adverse Events Study: the incidence of adverse events among hospital patients in Canada.
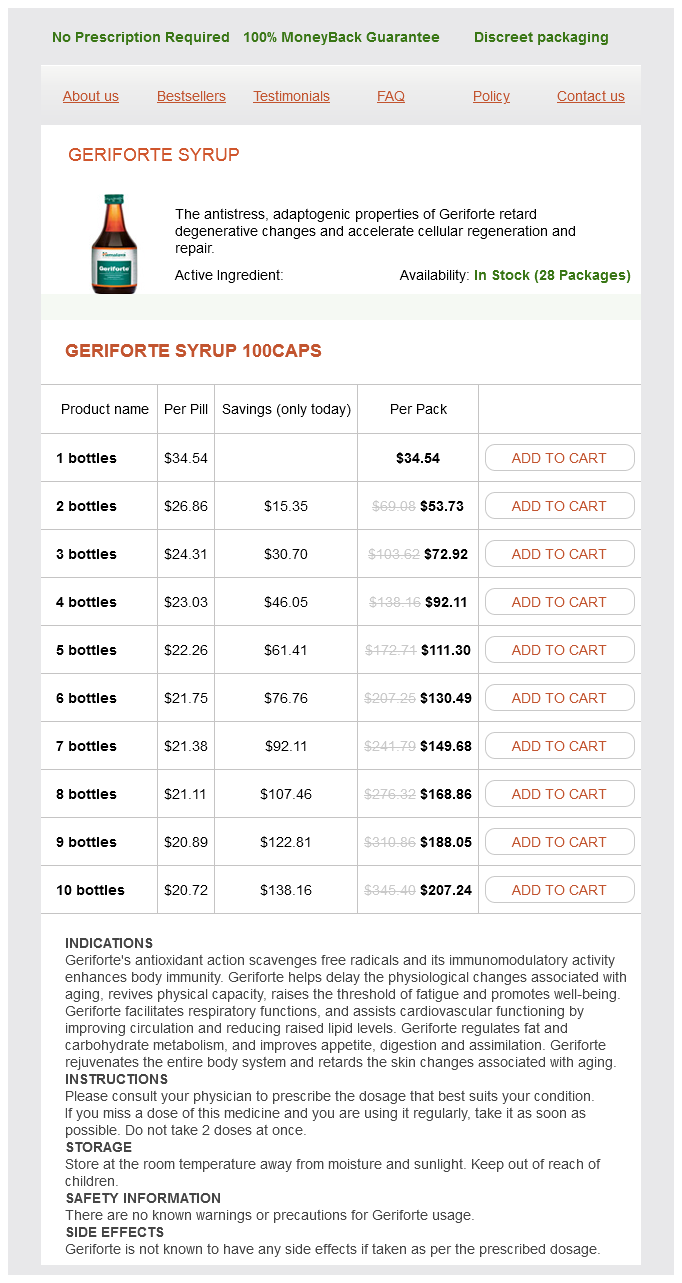
Geriforte Syrup Dosage and Price
Geriforte Syrup 100caps
- 1 bottles - $34.54
- 2 bottles - $53.73
- 3 bottles - $72.92
- 4 bottles - $92.11
- 5 bottles - $111.30
- 6 bottles - $130.49
- 7 bottles - $149.68
- 8 bottles - $168.86
- 9 bottles - $188.05
- 10 bottles - $207.24
Thus herbs de provence uses buy geriforte syrup 100 caps mastercard, following on from the above example, if the chain-shuffling patent is in force only in Europe, then the method may be carried out in India, but the patentee may well be able to prevent the import of the resulting antibodies into Europe. There has been much debate as to whether a method of screening antibodies to identify antibodies that have certain properties, for example, the ability to bind to a specific antigen, also provides protection for antibodies identified via the patented screening process. Uncertainty still exists and it is likely that not only will the courts of different countries arrive at different conclusions but also that decisions will be dependent on the specific facts of each case. For now, the key message is that it is important to be aware that method patents might provide powerful protection for patentees and represent key barriers for third parties. For example, a first patent may protect the antibody per se, a subsequent patent may protect a new medical application for the antibody and yet a further patent may protect a glycosylation variant of the antibody. Further layers may be introduced by seeking patent protection for production methods or for combination 25. If possible, it is a good strategy to try to obtain multiple layers of protection, and thereby to extend the period of protection for as long as possible. Consequently, no matter what the target antigen or the therapeutic application is, one or more relevant patents are likely to exist. It is therefore important for anyone working within this field to consider whether there are any infringement/ freedom-to-operate issues. The owner of a patent can take legal action against anyone carrying out unauthorized acts that are within the scope of their patent claims. The patent owner can try to impose an injunction, meaning that the infringing acts have to be stopped, and they can seek damages to compensate them for the losses incurred as a result of the unauthorized competition. A patentee can only bring infringement proceedings once a patent has granted, meaning that only granted patents can be enforced. This is because during the pendency of an application it is unknown what claim scope may eventually be granted. After the patent has granted, a patentee may bring infringement proceedings with regard to an infringement that took place during the pendency of the patent application, provided that the infringing act fell within the scope of the pending claims and within the scope of the claims that were eventually granted. In this regard, it is very important to appreciate that freedom to operate is solely determined by patents held by others. In other words, the grant of a patent allows the owner of the patent to prevent others from doing what is claimed in the patent. However, it does not give the owner any automatic right to exploit the patent himself. As mentioned above, patents are territorial rights, and therefore freedom to operate is a territorial issue, so a freedom-to-operate determination has to be made on a country-by-country basis. Many countries have laws that provide a ``research exception' (or ``research exemption') that permits the use of a patented invention for experimental purposes without infringing the rights of the holder. This typically applies only to acts done for experimental purposes relating to the subject matter of the invention. Consequently, it is generally not possible to determine whether specific acts fall within the research exemption without analyzing the relevant patents. In other words, it is necessary to determine which patents the acts might infringe and to analyze these patents to determine whether the research exemption applies. It is also worth noting that the scope of the exemption varies significantly between different countries, but as a general rule most commercial research activities are unlikely to benefit from this exemption. A more powerful exemption from infringement in relation to clinical trials and other activities carried out for obtaining marketing authorization exists in many countries. This exemption is commonly referred to as a bolar or clinical trials exemption and in the United States, it is also called the safe harbor. These types of exemptions were introduced in recognition of the fact that it can take many years to gather all of the data and information required to obtain marketing authorization for a medicinal product, and that preventing third parties from starting the process of generating this information during the lifetime of a patent would essentially have the effect of extending the monopoly period enjoyed by the patentee. It is important to note that the scope of the exemption varies widely from country to country. In Europe, a clinical trials exemption was introduced by way of a directive of the European Union, so one would be forgiven for assuming that European law is harmonized in this regard. In some European countries the exemption only applies to generic or ``biosimilar' medicinal products, whereas in other European countries the exemption extends to innovative medicinal products. Further differences relate, for example, to the issue of whether the trials are carried out in order to obtain marketing authorization within the European Union or outside of the European Union. There also remains uncertainty over the types of acts that fall within the exemption. It is therefore strongly recommended that legal advice be sought to determine whether and to what extent any of the exemptions from infringement apply to specific acts. Thus, while the laws of most countries provide certain exemptions from infringement, these exemptions may not necessarily be applicable to each specific case. In any event, for a commercially important project it would generally be recommended to carry out at least a basic freedom-to-operate analysis relatively early in the life cycle of the project in order to identify patents that might be potential barriers to commercialization. Both the search and the subsequent analysis require specialist skills, so it is best to seek professional assistance, for example, from a patent attorney. As explained above, patents are territorial rights, so it is necessary to determine in which countries the desired activities are proposed to take place and to tailor the search accordingly. In the field of therapeutic antibodies, although it may be desirable to market the antibody worldwide, owing to cost considerations, it can be a good idea to start with a limited search, and to consider widening the scope of the search at a later stage. In particular, a pragmatic approach may be to limit the initial search to Europe and the United States.