General Information about Fluoxetine
Fluoxetine could interact with other drugs, including different antidepressants, blood thinners, and drugs for coronary heart situations, so it is essential to tell the prescribing physician of another medicines being taken. It can be necessary to avoid alcohol and recreational drugs while taking fluoxetine, as they might enhance the chance of side effects and intrude with the medication's effectiveness.
In addition to despair, fluoxetine can be generally prescribed for the treatment of OCD. This is a dysfunction during which people wrestle with uncontrollable and recurring thoughts (obsessions) and repetitive behaviors (compulsions) that intrude with day by day life. It is believed that fluoxetine helps to alleviate signs of OCD by regulating the degrees of serotonin in the mind, leading to a reduction in obsessive and compulsive behaviors.
In conclusion, fluoxetine is a widely prescribed medicine that has proven to be an effective remedy for depression and OCD in adults. By balancing serotonin ranges within the brain, it might possibly improve mood and reduce symptoms of those mental well being circumstances. However, it is essential to use it as prescribed and follow the physician's instructions to make sure protected and efficient treatment. With correct remedy and help, individuals can discover reduction from the signs of despair and OCD and enhance their total high quality of life.
When prescribed fluoxetine, you will need to observe the doctor's directions intently and attend scheduled follow-up appointments to monitor its effectiveness. It might take as much as 4-6 weeks for the treatment to achieve its full impact, so persistence and consistency with taking the treatment are key. In addition to treatment, therapy and different types of assist, corresponding to help teams, may be beneficial to assist in the administration of melancholy or OCD.
Fluoxetine, also identified by its model name Prozac, is a commonly prescribed treatment used to treat melancholy and obsessive-compulsive dysfunction (OCD) in adults. As a selective serotonin reuptake inhibitor (SSRI), it really works by balancing chemical imbalances within the brain, improving temper and conduct.
Depression is a serious and common psychological illness that affects tens of millions of individuals worldwide. It is characterised by emotions of disappointment, loss of curiosity in daily activities, and changes in sleep and urge for food. While it can be triggered by a wide range of factors, similar to genetics, life occasions, or chemical imbalances within the brain, it is a treatable situation. Fluoxetine works by rising the degrees of serotonin, a chemical messenger in the mind that is responsible for regulating temper, in order to alleviate symptoms of despair.
As with any medicine, fluoxetine might trigger side effects. Common unwanted effects embody nausea, dizziness, headache, insomnia, and modifications in appetite and weight. These unwanted effects are usually temporary and can subside as the physique adjusts. However, in the event that they persist or turn out to be bothersome, you will want to seek the assistance of a physician. In rare cases, fluoxetine can also result in extra extreme side effects, corresponding to allergic reactions or suicidal ideas. It is essential to seek medical consideration immediately if any of those signs happen.
Fluoxetine comes in the type of capsules, tablets, and an oral resolution, and is normally taken as quickly as a day within the morning. The dosage prescribed will vary relying on the individual's age, medical history, and severity of symptoms. It is necessary to follow the prescribed dosage and continue taking the treatment even when signs improve, as abruptly stopping the medicine can lead to withdrawal signs and a possible relapse of melancholy or OCD.
Perceived susceptibility to breast cancer moderates the effect of gain and lossframed messages on use of screening mammography women's health xmas kekse cheap fluoxetine online visa. Promoting the avoidance of highcalorie snacks: Priming autonomy moderates message framing effects. Approach/avoidance motivation, message framing, and health behavior: Understanding the congruency effect. Message framing for health: Moderation by perceived susceptibility and motivational orientation in a diverse sample of Americans. The effects of message quality and congruency on perceptions of tailored health communications. The cultural congruency effect: Culture, regulatory focus, and the effectiveness of gain vs. Health message framing effects on attitudes, intentions, and behavior: A metaanalytic review. The strategic use of gainand loss framed messages to promote healthy behavior: How theory can inform practice. Most people recognize risks associated with these unhealthy behaviors and the potential benefits of adopting healthy behaviors in lowering their risk for chronic illness. Yet many continue to make unhealthy lifestyle choices even when they experience undesired consequences for their actions (or inaction) or even if they have a genetic predisposition toward a particular chronic disease (King, Mainous, Carnemolla, & Everett, 2009). Health psychologists recognize that a number of factors can shape health behaviors and that these factors vary from one individual to another. Health messages primarily designed to raise awareness without considering the complexity of behavior change are deemed to have limited impact on individual actions and decision making. It is for this reason that interpersonal communication continues to be the ideal channel for promoting individual behavior change because of the ability to adjust communication on the fly and to deliver personalized recommendations. Unfortunately, the reach and accessibility of health counselors adequately trained in delivering evidencebased personalized recommendations is limited. Message tailoring, a health communication strategy for disseminating theoretically informed individualized recommendations, seeks to address this need to deliver more efficacious health behavior change strategies on a mass scale. The Tailoring Process Message tailoring is defined as a "multidimensional communication strategy that involves developing individualized messages based on a preassessment of key individualdifference the Wiley Encyclopedia of Health Psychology: Volume 2: the Social Bases of Health Behavior, First Edition. Information about the individual is typically assessed through a survey of relevant factors. This data is then evaluated by an expert system that uses tailoring algorithms to prioritize content and recommendations based on user input. At the most basic level, this process involves selecting messages most relevant for the individual from a database of tailored content. A typical tailoring system includes (a) a way to collect information about the individual. It is not to be mistaken for simple personalization or the inclusion of personal identifiers, the main goal of which is to draw attention to the health message. It is also different from targeted messaging or creating messages that might resonate with specific groups of people that share common characteristics. Rather, in tailored messaging, individuallevel assessment enables the creation and delivery of highly personalized recommendations and plans for modifying simple to complex health behaviors based on an analysis of individual drivers for (and barriers to) change. As people age, their body composition gradually shifts - the proportion of muscle decreases and the Message Tailoring 365 proportion of fat increases. In addition, some people become less physically active as they get older, increasing the risk of weight gain. The good news is that choosing a lifestyle that includes good eating habits and daily physical activity can prevent weight gain. In contrast, the following is an example of how a tailored health message differs from the generic message just provided: Hi Pam! Based on your current age, weight and height, you are slightly at risk for obesity. This extra weight can but stress on your bones, joints, and organs, which may partly explain your lethargy and difficulty in sustaining your daily activities. Too much body fat also raises your blood pressure and cholesterol this can be very dangerous for people like you who have a family history of heart disease and stroke. Being a busy career woman and mom, we understand that this is easier said than done. Message Tailoring Works A wide evidence base promotes the use of tailored messaging over onesizefitsall generic messaging. Compared with nontailored messages, tailored information commands greater attention and is processed more intently, recalled more readily, and perceived as more personally relevant and more positively by health consumers (Kreuter, Strecher, & Glassman, 1999). More importantly, several studies and metaanalyses provide empirical evidence for the benefits of tailored versus nontailored interventions across a wide variety of health outcomes such as physical fitness, nutrition, mental health, immunization, early detection or screening, sexual health, alcoholism, and chronic disease. Overall, various metaanalyses have pointed to small and mediumsize effects of tailoring on behavior change. Noar, Benac, and Harris (2007) conducted a metaanalytic review of 57 tailored print behavior change interventions and found a mean effect of r =. The variables that were found to significantly moderate the effect included (a) type of comparison condition, (b) health behavior, (c) type of participant population (both type of recruitment and country of sample), (d) type of print material, (e) number of intervention contacts, (f) length of followup, (g) number and type of theoretical concepts tailored on, and (h) whether demographics and/or behavior were tailored on. Krebs, Prochaska, and Rossi (2010) also conducted a metaanalysis to evaluate the mean effect of 88 computertailored interventions focusing on smoking cessation, physical activity, eating a healthy diet, and receiving regular mammograms. They found clinically and statistically significant overall effects across each of the four behaviors. Effect sizes decreased after intervention completion, and dynamically tailored interventions were found to have increased efficacy over time as compared with those based on one assessment only.
However women's health center fremont ca cheap fluoxetine 10 mg without prescription, the body can detect this stress state and effectively respond by mounting a coordinated stress response. Despite the various theoretical conundrums surrounding the nature of this stress state, researchers have made a number of important discoveries concerning the neurobiology of stress. Types of Stressors the categorization of stressors into two general types, physiological and psychological, has proven useful for studying the specific underlying neurocircuitry that participates in the processing and response coordination to these stressors. Physiological stressors are those altered physiological states that elicit wellcharacterized autonomic homeostatic adjustments, such as hypothermia, hypoxia, dehydration, tissue damage, hypotension, and hemorrhage. Some of these socalled psychological (or processive) stressors are environmental stimuli that appear to be innately recognized as an immediate threat to physiological wellbeing, such as physical attack, sudden loud noise, impending collision with a fast moving object, or teetering on the edge of a high precipice. However, physiological stress responses are also effectively triggered by many other experiential situations that do not reflect impending bodily harm, such as public speaking, novel social circumstances, traffic jams, relationship difficulties, financial insecurity, and job performance concerns. Research has identified several underlying psychological factors that are shared by various psychosocial situations that are considered stressful, and these factors include lack of controllability, lack of predictability, novelty, and socialevaluative threat. The ability to respond to psychological stressors with a physiological stress response confers considerable adaptive advantage to the organism. If the organism is able to initiate a physiological stress response not only to a direct physical insult. The ability not only to respond to immediate physical stressors but also to anticipate and prepare for future stressors is a key aspect of evolutionary stress neurobiology. However, in modern society, many complex psychosocial stressors are not Neurobiology of StressHealth Relationships 23 associated with impending physical threat to wellbeing, and consequently the activation of physiological stress responses in these situations is not adaptive and contributes to the adverse effects of chronic stress on health. Types of Stress Responses Physiological and psychological stressors elicit not only a physiological response but also psychological responses. The psychological responses often include generation of emotional states, such as fear, anxiety, or frustration, as well as shifts in attention. This psychological aspect of the stress response is essential for motivation and coordination of adaptive behavioral responses. No physiological or psychological response alone, or in combination, is a dedicated response exclusively reserved for combatting stress. Each can occur in other contexts, and therefore the presence of these responses is not a definitive measure of stress, although they may be useful biomarkers associated with stress. However, because there is not a physical dimension of stressfulness inherent in stimuli, the determination of stressfulness or threat requires integrative neural processing. The perception of and the coordinated response to stress depend on hierarchically organized neural systems in the brain. In the case of an appropriate response to physiological stressors, the underlying neural circuitry tends to be relatively simple. For example, a sudden drop in blood pressure results in reduced activity of baroreceptors located in the aortic arch and carotid artery sinus. These specialized sensory neurons project via the vagus and glossopharyngeal cranial nerves to the vasomotor control centers in the brain stem. Superimposed on these evolutionarily primitive neurocircuits are more complex neural circuits and networks. The two systems mediate complementary adaptive changes in virtually every cell and system of the body, and both systems operate on a complementary time scale. Individuals do not have voluntary control over the initiation or termination of activity within these two stress response systems, but they may learn strategies, such as relaxation techniques to modulate their activity. Also depicted is an example of sympathetic postganglionic neuron projections to skin and a section of a blood vessel, where norepinephrine is released from nerve terminals. Neurobiology of StressHealth Relationships 25 system, bladder, reproductive organs, salivary glands, and lacrimal glands. Axons of the preganglionic sympathetic neurons extend outside the spinal cord to synapse onto postganglionic cell bodies, many of which are located in sympathetic chain ganglia adjacent to the spinal column. The axons of postganglionic neurons terminate on target organs throughout the body. Preganglionic neurons release acetylcholine onto nicotinic cholinergic receptors present on postganglionic neurons, while postganglionic neurons release norepinephrine onto adrenergic receptors present on target organs. Norepinephrine release onto target organs triggers physiological changes associated with the fightorflight response, including pupil dilation, shunting of blood flow from the viscera to the skeletal muscles of the limbs, increased respiration, and heart rate acceleration. The axons of sympathetic preganglionic neurons in the thoracic spinal cord extend as part of the splanchnic nerve to terminate on chromaffin cells. Chromaffin cells, in response, secrete the catecholamine molecules epinephrine (also known as adrenaline) and norepinephrine into the systemic circulation. Catecholamine hormones cannot cross the bloodbrain barrier and therefore act only in the periphery, with epinephrine binding all classes of adrenergic receptors (1, 2, 1, 2, and 3 adrenergic receptors) and norepinephrine binding preferentially 1, 2, and 1 adrenergic receptors. Given the different receptor binding affinities of epinephrine and norepinephrine and the differential distribution of adrenergic receptor subtypes on target organs throughout the periphery, epinephrine and norepinephrine generate different effects. Epinephrine, for instance, is particularly effective in increasing heart rate, cardiac output, and blood glucose, while norepinephrine is most effective in increasing blood pressure and energy mobilization by breaking down fats (lipolysis). These neurons project to a region at the base of the hypothalamus (median eminence) that forms the junction between the brain and the pituitary stalk. These neurons are called hypophysiotropic neurons because they project to the interface region between the brain and pituitary (also known as hypophysis). The second population of cells consists of endocrine cells, called corticotrophs, located in the anterior pituitary. The third population of cells consists of endocrine cells located in the outer cortex (fasciculata layer) of the adrenal gland.
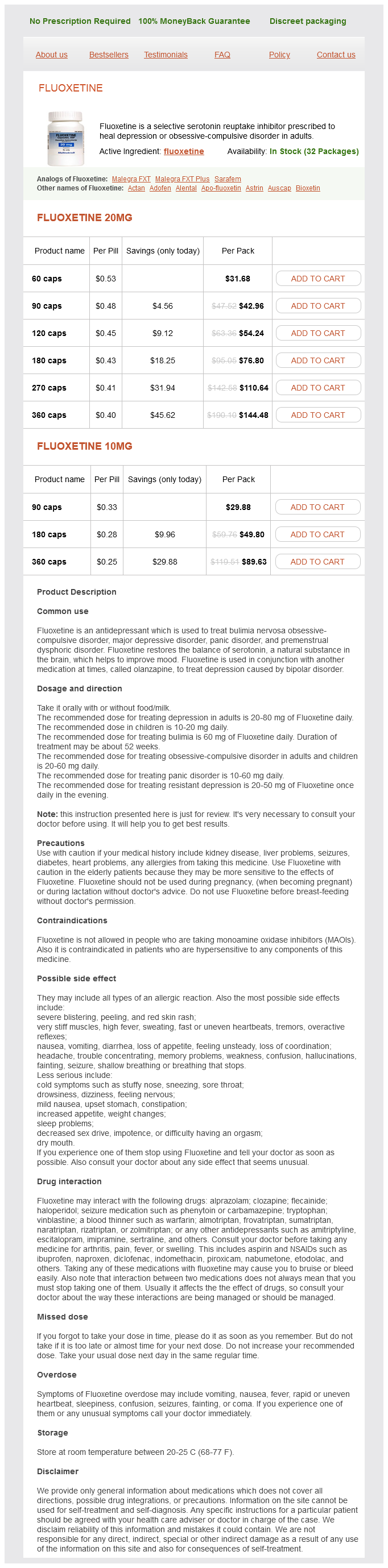
Fluoxetine Dosage and Price
Fluoxetine 20mg
- 60 caps - $31.68
- 90 caps - $42.96
- 120 caps - $54.24
- 180 caps - $76.80
- 270 caps - $110.64
- 360 caps - $144.48
Fluoxetine 10mg
- 90 caps - $29.88
- 180 caps - $49.80
- 360 caps - $89.63
Longitudinal associations among posttraumatic stress disorder symptoms women's health center reno order fluoxetine 20 mg without prescription, traumatic brain injury, and neurocognitive functioning in army soldiers deployed to the Iraq war. Traumatic brain injury and posttraumatic stress disorder: Conceptual, diagnostic, and therapeutic considerations in the context of cooccurrence. Reduced hippocampal volume and total white matter volume in posttraumatic stress disorder. Biased emotional attention in posttraumatic stress disorder: A help as well as a hindrance Multisite investigation of traumatic brain injuries, posttraumatic stress disorder, and self reported health and cognitive impairments. Among the lifestyle characteristics examined, physical activity and dietary practices have been most extensively studied (Scarmeas et al. In addition, several lines of evidence among humans suggest that more limited intake of energy may confer reduced risk of dementia. Similarly, several randomized trials have provided evidence, albeit preliminary, that intentional caloric restriction may improve cognitive performance (Witte, Fobker, Gellner, Knecht, & Floel, 2009) and improve neuroimaging markers of brain health (Espeland et al. Nevertheless, multiple studies have suggested that lower weight, particularly underweight, is associated with worse outcomes among older adults, in contrast to the protective effects demonstrated in midlife. Smith Epidemiological Data Accumulating evidence suggests that lower levels of caloric intake may be associated with improved cognitive performance and reduced rates of dementia. Although several recent examinations have been conducted in humans, this relationship has been studied extensively among animals. Despite relatively limited evidence in humans linking caloric restriction directly to brain outcomes, multiple, indirect lines of evidence support the notion that restricted energy intake may have salubrious effects. For example, multiple studies have demonstrated that being overweight or obese, particularly in midlife, is a risk factor for dementia (Kivipelto et al. Although the mechanisms linking obesity to dementia are likely multifactorial (Craft, 2009), recent studies have suggested that the presence of obesity in midlife is associated with neuropathological correlates of dementia, including neurofibrillary tangles (Chuang et al. Despite these findings, it must also be noted that not all studies have shown an association between obesity and increased risk of dementia, a phenomenon that has come to be referred to as the "obesity paradox" (Driscoll et al. Independent of studies examining obesity, a separate line of evidence suggests that more modest caloric intake is associated with improved longevity and that excess energy intake is associated with adverse cognitive outcomes. A wellknown association has also been documented between chronic, markedly diminished caloric intake and improved longevity among Okinawans, who have a high prevalence of centenarians and relatively low rates of dementia (Willcox et al. In an archival analysis of centenarian Okinawans, participants even reported a 10. Randomized Trials Relatively few randomized trials have directly tested the impact of caloric restriction in human participants. Following 3 months of treatment, individuals in the caloric restriction group exhibited increased verbal memory scores, and these improvements were correlated with decreased levels of fasting insulin and Creactive protein. Participants were randomly assigned to one of four groups: caloric restriction, caloric restriction and exercise, a lowcalorie diet condition, or to a control group (weight maintenance). At baseline, 3 months, and again at 6 months, cognitive tests were administered assessing verbal and visual memory, as well as concentration/attention. Overall, cognitive function changed very little across any group, and no consistent pattern of change emerged. In addition, changes in cognitive performance were not related to changes in caloric intake (indexed by daily energy deficit) or weight loss. Several other randomized trials provide preliminary evidence that caloric restriction may confer cognitive and/or brain benefits in various patient populations. We previously examined this relationship in a sample of 120 middleaged adults with hypertension and overweight or obesity (Smith et al. In one of the longest randomized trials to examined caloric restriction, Espeland et al. In order to examine this relationship, the authors conducted a per protocol analysis, incorporating only individuals who exhibited at least modest weight loss. At the time of the 10year followup, participants in the intervention group exhibited 28% lower white matter volume compared with control participants, who underwent a diabetes support and education program. In contrast, improvements in cognitive performance were relatively modest, only being observed on one subtest of processing speed. In a per protocol analysis, the authors excluded individuals in the intervention group who did not lose at least 10% body weight, as well as participants in the control group who lost more than 5% of body weight. Participants in the intervention group exhibited improved memory performance paralleled by increased gray matter volume in the inferior frontal gyrus and hippocampus, as well as augmented hippocampal restingstate functional connectivity to parietal areas. The effects appeared to be specific to transient negative energy balance and were not detected after subsequent weight maintenance. An overlapping but conceptually distinct question is whether weight loss is associated with improvements in neurocognitive performance. Although many studies achieve weight loss through a combination of exercise and dietary modification, more modest weight loss may be achieved through exercise alone. In addition, some studies have examined the impact of weight loss through bariatric surgery and its impact on cognitive change, although these studies are beyond the scope of the present review. In one of the few systematic reviews to examine intentional weight loss and cognitive function changes, Siervo et al. Smith majority of studies included were behavioral weight loss interventions, gastric bypass studies were also included.