General Information about Finasteride
Aside from its effectiveness in treating male pattern baldness, finasteride has additionally been confirmed to be helpful for men with prostate cancer. The medicine works in an identical means for each hair loss and prostate cancer because it blocks the conversion of testosterone to DHT. This, in flip, slows the expansion of most cancers cells in the prostate gland. Finasteride is commonly prescribed in combination with different remedies for prostate cancer.
When used for hair loss, finasteride is beneficial for males between the ages of 18 to forty one, because it has not been confirmed to be effective for men over forty one. It can additionally be not recommended for use in girls, notably pregnant ladies, as it could probably trigger harm to a developing male fetus.
As with any treatment, there are some potential unwanted aspect effects of finasteride. The commonest unwanted side effects include decreased libido, erectile dysfunction, and decreased ejaculation volume. However, these unwanted effects are uncommon and normally resolve once the medication is stopped. It is necessary to talk to a physician if you experience any regarding unwanted facet effects while taking Propecia.
Finasteride is a prescription medicine that was initially developed to deal with benign prostatic hyperplasia (BPH), a common condition in men the place the prostate gland becomes enlarged. However, it was discovered that the drug also had a big impact on hair development in men with male pattern baldness. This led to the event of Propecia – the first and only FDA-approved medicine to deal with male pattern hair loss.
Male pattern hair loss, also called androgenic alopecia, is a hereditary situation that impacts roughly 50 million males in the United States alone. It is characterized by a receding hairline and thinning of hair on the crown of the pinnacle. This kind of hair loss is brought on by the hormone dihydrotestosterone (DHT), which is a byproduct of testosterone. DHT causes hair follicles to shrink, resulting in shorter and finer hair, eventually leading to hair loss. Finasteride works by inhibiting the conversion of testosterone to DHT, thus lowering the quantity of DHT within the body and permitting hair follicles to regain their normal measurement.
Propecia comes in the type of a tablet to be taken orally as quickly as a day. Studies have proven that it's effective in slowing hair loss and selling new hair growth. In fact, in a five-year medical study, over 90% of males who took Propecia experienced a rise in hair progress on their scalp. Results can typically be seen within three to 6 months of starting treatment and further improvement can continue for as a lot as two years.
In today’s fast-paced world, physical look has turn out to be extra essential than ever. It is not any shock that hair loss, particularly in males, is a significant concern and may have a big influence on shallowness and confidence. Fortunately, medical advances have made it potential to treat male pattern hair loss effectively with the assistance of a medicine called finasteride, also referred to as Propecia.
In conclusion, finasteride, generally generally recognized as Propecia, is a extremely effective medication for the remedy of male sample hair loss. It has been a game-changer for tens of millions of males worldwide, providing them with a safe and dependable solution to combat hair loss and promote healthy hair development. However, you will need to consult with a doctor to determine if this treatment is the proper choice for you and to watch any potential unwanted aspect effects. With the help of finasteride, many males can now feel extra confident and comfortable in their own pores and skin and have one much less factor to worry about.
British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of rheumatoid arthritis (after the first 2 years) hair loss miracle cure order finasteride cheap online. Evaluation of diagnostic criteria for ankylosing spondylitis: a proposal for modification of the New York criteria. Comparison of recommendations for the use of anti-tumour necrosis factor therapy in ankylosing spondylitis in 23 countries worldwide. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. Guidelines of care for the treat ment of psoriasis and psoriatic arthritis: case-based presenta tions and evidence-based conclusions. Guidelines of care for the man agement of psoriasis and psoriatic arth ritis: section 4. Guide lines of care for the management and treatment of psoriasis with traditional systemic agents. Point: Hydroxyapatite crystal deposition is intimately involved in the pathogenesis and pro gression of human osteoarthritis. Counterpoint: Hydroxyapatite crystal deposition is not intimately involved in the pathogenesis and progres sion of human osteoarthritis. European League Against Rheu matism recommendations for calcium pyrophosphate deposi tion. Part I: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Viscosupplementation for osteoar thritis of the knee: a systematic review of meta-analysis. Differentiation of post-strepto coccal reactive arthritis from acute rheumatic fever. Hereditary hemochromatosis: a neglected diagnosis in orthopedics: a series of 7 patients with ankle arthritis, and a review of the literature. Pathogenic Neisseriae: gonorrhea, neonatal ophthal mia and meningococcal meningitis. European League Against Rheumatism recommendations for monitoring patients with systemic lupus erythematosus in clinical practice and in observational studies. Mixed connective tissue disease: an overview of clinical manifestations, diagnosis and treatment. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Antiphospholipid syndrome: laboratory detec tion, mechanisms of action and treatment. Committee on Practice Bulletins-Obstetrics, American College of Obstetricians and Gynecologists. SpringerLink (Online service), International Congress on Antiphospholipid Antibodies, Erkan, D. Antiphospholipid syndrome: Insights and highlights ji-om the 13th International Congress on Antiphospholipid Antibodies. Antiphospho1ipid syndrome: laboratory detection, mechanisms of action and treatment. Nailfold capillaroscopy is useful for the diagnosis and follow-up of autoimmune rheumatic diseases. Systemic sclerosis - a systematic over, view: part I - disease characteristics and classification, patho physiologic concepts, and recommendations for diagnosis and surveillance. Treatment of systemic sclerosis complications: what to use when first-line treatment failsa consensus of systemic sclerosis experts. Giant cell arteritis: a review of classification, pathophysiology, geoepidemiology and treat ment. Epidemiology and etiology of Wegener granulomatosis, microscopic polyangiitis, Churg-Strauss syndrome and Goodpasture syndrome: vasculitides with frequent lung involvement. Aortitis: imaging spectrum of the infectious and inflammatory conditions of the aorta. Large- and small-vessel vasculitis: a critical digest of the 2010-2011 literature. Review of current therapies for second ary hypertrophic pulmonary osteoarthropathy. Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians. Examination of the elbow: linking diagnosis, prognosis, and outcomes as a framework for maximizing therapy interventions. Medications for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physi cians clinical practice guideline. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American Col lege of Physicians and the American Pain Society. Comprehensive evi dence-based guidelines for interventional techniques in the management of chronic spinal pain. We at MedStudy do our best to review and include in this publication accurate discussions of the standards of care and methods of diagnosis.
This is a difficult regimen to comply with and water alone is often ineffective when urinary cystine excretion exceeds 500 mg/day hair loss and thyroid buy discount finasteride 5 mg online. Alkalinization is a secondary measure used in those who do not respond to water alone. Potassium citrate is preferable to sodium citrate or bicarbonate as extracellular fluid volume expansion that occurs with sodium salts increases urinary cystine excretion. D-Penicillamine or tiopronin (-mercaptopropionylglycine) is used if water and alkali are ineffective. They are almost always required in patients with high urinary cystine excretion (>1000 mg/day). These drugs are thiols that bind to cysteine and form compounds that are more soluble in aqueous solution than cystine. In one nonrandomized trial, 31% of patients stopped therapy because of unacceptable side effects with tiopronin versus 69% of those on D-penicillamine. D-Penicillamine binds pyridoxine and pyridoxine (50 mg/day) should be administered to prevent deficiency. Zinc supplements help prevent the anosmia and loss of taste that can occur with D-penicillamine. The dose of tiopronin is 400 to 1200 mg daily in 3 to 4 divided doses, whereas the D-penicillamine dose is 0. Captopril was initially reported to be of benefit, but subsequent studies have not borne this out. Monitoring drug therapy is complicated by the fact that some urinary assays cannot distinguish between free cystine and cysteine complexed to D-penicillamine or tiopronin. The amino acid cysteine dimerizes to form cystine that has limited solubility in water (250 mg/L). Water is the hallmark of treatment but is often of limited use in patients who excrete more than 500 mg of cystine. Ancillary measures include alkalinization of the urine with potassium citrate, and agents that form dimers with cysteine including tiopronin (-mercaptopropionylglycine) and D-penicillamine. Of the sulfa drugs, sulfadiazine is more likely to precipitate than sulfamethoxazole. This occurs most commonly after several days of high-dose therapy for Toxoplasmosis gondii or Pneumocystis carinii infection and presents as acute kidney injury. Treatment involves discontinuation of the drug, alkalinization of the urine to pH greater than 7. Triamterene is a weak base that can precipitate and form stones in the urinary tract. In one series, 22% of reported stones contained only triamterene, 14% had more than 90% triamterene, and 42% had less than 20% triamterene mixed with calcium oxalate and uric acid. The annual incidence was estimated at 1 in 1500 patients among those prescribed the drug. Triamterene should be avoided in patients with a previous history of calcium oxalate or uric acid stones. Acyclovir use can result in crystal-induced acute kidney injury, especially if the drug is infused rapidly intravenously or the dose is not adjusted for renal dysfunction. The incidence is reduced by slow infusion over 1 to 2 hours with vigorous prehydration. There are rare case reports of acute kidney injury with oral therapy in those who were dehydrated or received too high a dose. Cystinuria is secondary to an autosomal recessive defect in proximal tubular and jejunal reabsorption of dibasic amino acids. Nephrolithiasis develops in 3% of patients, and 5% will experience either dysuria or flank pain that resolves when the drug is discontinued. Nelfinavir, saquinavir, atanazavir, and efavirenz may also crystallize in the urine and cause stones. This results from abuse of nonprescription cold formulations or the ingestion of Ma-huang. Ma-huang is rich in ephedrine, norephedrine, pseudoephedrine, and norpseudoephedrine. Observational studies suggest an association of nephrolithiasis and chronic kidney disease. Whether this is a result of confounders or renal injury from stone disease remains to be determined. A variety of prescriptions and nonprescription drugs can precipitate in urine and form stones. A careful medication history should be a part of the evaluation of all patients with nephrolithiasis. A series of stone formers from France showed an increased incidence of end-stage renal disease. A high percentage of these patients had struvite stones that are known to be associated with loss of renal function. Whether this can be explained by the high incidence of hypertension and diabetes in these patients or is a result of the stone disease itself is unclear. Potential pharmacologic treatments for cystinuria and for calcium stones associated with hyperuricosuria. Thiazides diuretics in the treatment of nephrolithiasis: are we using them in an evidence-based fashion What information does the urinalysis/urine microscopy provide about patients with kidney disease What information does the presence of cellular casts in the urine sediment provide Is the presence of uric acid or calcium oxalate crystals always indicative of a defined renal disease Is the random spot urine protein-to-creatinine ratio an accurate estimate of daily protein excretion Do patterns of urinary findings help differentiate various types of kidney disease Does quantitative examination of the urine sediment improve diagnosis and allow prognosis in patients with acute tubular necrosis Kidney disease is fully assessed with complete history and physical examination, directed blood testing, and examination of the urinary sediment. This chapter reviews the components of the urinalysis/ urine microscopy, as well as their interpretation in patients with kidney disease.
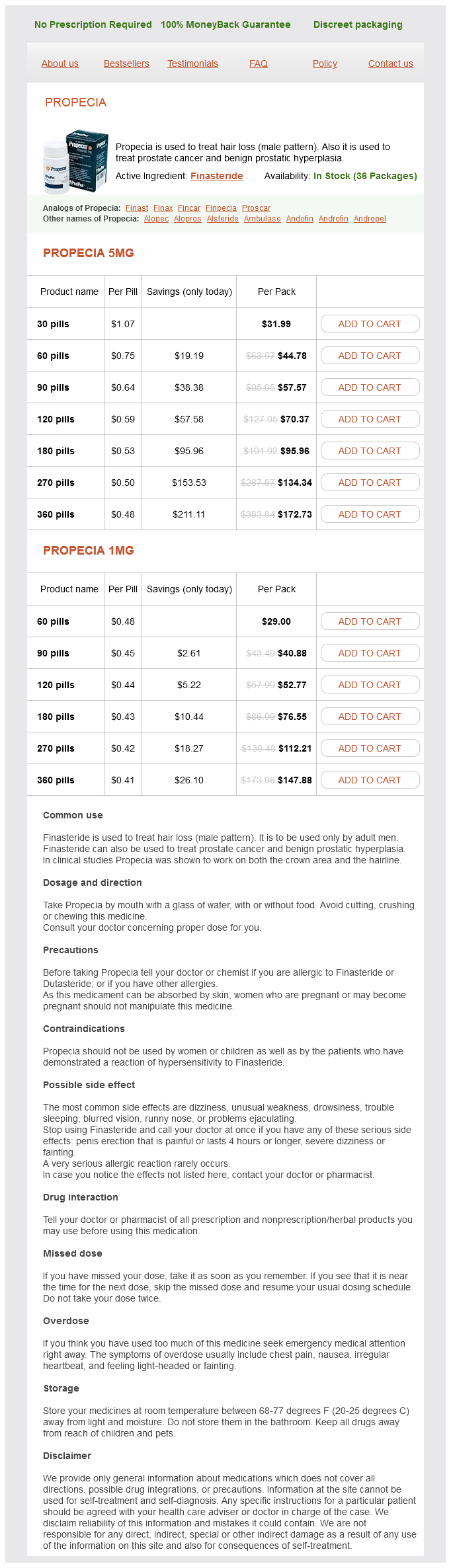
Finasteride Dosage and Price
Propecia 5mg
- 30 pills - $31.99
- 60 pills - $44.78
- 90 pills - $57.57
- 120 pills - $70.37
- 180 pills - $95.96
- 270 pills - $134.34
- 360 pills - $172.73
Propecia 1mg
- 60 pills - $29.00
- 90 pills - $40.88
- 120 pills - $52.77
- 180 pills - $76.55
- 270 pills - $112.21
- 360 pills - $147.88
Concerns about the new lung cancer screening proposal center around the potential of overdiagnosis hair loss yasmin discount 5 mg finasteride free shipping, excess radiation exposure, and cost. However, the evidence would suggest that I lung cancer death is averted for every 450-500 scans done. Tobacco avoidance and cessation continue to be important steps in decreasing the burden of disease. It is a health care delivery and reimbursement model that ties the reimbursement to the quality of health care delivered and the total cost of care. Example: 4 regional hospitals combine their outpatient services to better serve the local population. Primary care physicians and specialists from each of the 4 hospi tals participate. The costs of the services are bundled to meet predetermined budgets, which include incentives to meet specific performance improvement objectives. About 80% of fatal overdoses were unintentional, and prescription drugs accounted for the majority of deaths! Opioids were the most common drugs involved, often found in combination with benzodiazepines. These events, and increased osmolar gaps are covered exhaustively in Nephrology, Book 2. Assessment of airway is most important, with immediate intubation of the patient with unstable vital signs and/or inability to protect the airway. The following interventions are usually empirically performed, except as noted: · with "excitation" or "depression" and know which ingestions are associated with the presented scenarios (Table I 0-11). In clinical practice, many patients present with co-ingestions, and the physical exam can be a mixed bag of signs/symptoms. Tip: mydriasis = dilated pupils (big word, big pupils); miosis= constricted pupils (small word, small pupils). Know that acti vated charcoal is not effective when the overdose is with the metals lithium and iron. Continued dosing with oral charcoal is effective in decreasing the levels of a few drugs by gut dialysis (absorption via the enteric recirculation)-especially digoxin, phenobarbital, theophylline, tricyclics, and salicylates. The thought is that lavage is, in most cases, ineffective; using activated charcoal with cathartics is at least as effective, if not more so. Alkalinization and acidification of the serum (and hence, the urine) are based on the principle that com pounds in their ionized form are less tissue-permeable and more easily eliminated by the kidneys. Weakly acidic substances ionize in an alkaline environment while weakly alkaline substances ionize in an acidic environment. Important: Hemodialysis may be necessary in patients with severe overdose or renal failure. It is effective in removing drugs with low molecular weights that are not lipid soluble, protein bound, or tissue bound-i. These include lithium, chloral hydrate, salicylates, and alcohols (meth anol and ethylene glycol). Also important: Charcoal hemoperfusion (blood pumped through a charcoal filter), in contrast to dialy sis, removes drugs that are lipid soluble and protein bound! Also, like dialysis, it is most effective in removing drugs with a low volume of distribution (V). Charcoal hemoperfusion is especially good for digoxin, theophylline, and salicylate overdoses. Iron Carbon monoxide Ethylene glycol Methanol Organophosphates Cyanide Nitrates, Na-thiosulfate volume), decreased bowel sounds, and constricted pupils. Know that meperidine, propoxyphene, and tramadol are associated with seizures in intoxicated patients (espe cially those on dialysis! The drug should be used to reverse hypoventilation induced by opiates-it should not be used in large doses as a diagnostic tool for opiate intoxi cation because of the risk of inducing withdrawal in the chronic user. The dose of naloxone should be titrated to result in normal ventilation (I 0-14 breaths/minute), not consciousness. Too great of a dose (enough to wake someone up completely) can cause rapid reversal and withdrawal. Chronic users of opiates, and those patients who inhaled or ingested a large dose of the drug, may require an intravenous drip of naloxone because its half-life is very short. Generally, 2/3 of the dose that results in adequate ventilation is given per hour in a drip. Know that acute lung injury is sometimes seen in opiate addicts who undergo rapid reversal of unconsciousness with naloxone+ high-flow oxygen via facemask. Also recognize that naloxone is typically not the correct answer if a scenario presents a patient with dilated pupils. Salicylates agents and their Analgesics Opiates Salicylates are metabolized in the liver by conjugation with glycine or glucuronide. These pathways are quickly saturated in a person who has overdosed, resulting in acidemia. Acidosis can worsen if Opioid prescriptions increased 700% from the years 1997 to 2007. Of the 22,000 deaths from prescription drugs in 20I 0, 75% involved opioid analgesics! If the patient stops hyperventilating, it is probably due to respiratory muscle fatigue. Even when given late in the course to a patient with significant ingestion and toxicity, it reduces mortality and improves liver func tion.