General Information about Eurax
Aside from treating scabies, Eurax is also used as a secondary treatment for different pores and skin situations, similar to eczema, dermatitis, and bug bites, to alleviate itching and irritation. It is on the market over-the-counter in most pharmacies, and a doctor's prescription just isn't required to purchase it.
If left untreated, scabies can lead to a secondary an infection, similar to impetigo or cellulitis, which could be more severe. Therefore, it's crucial to hunt immediate therapy as soon as scabies is suspected. European guidelines advocate using Eurax because the first-line therapy for scabies, as a result of its effectiveness and low danger of unwanted aspect effects.
In conclusion, Eurax is an antipruritic and scabicidal medication extensively used for treating scabies and relieving itching. It works by killing scabies mites and soothing the pores and skin. It is available over-the-counter, and whereas it is generally secure and efficient, it's essential to observe correct application and hygiene tips. If you think you might have scabies, seek the advice of a healthcare skilled for proper prognosis and remedy, including the use of Eurax.
In common, Eurax is taken into account a secure and efficient treatment for scabies and other pores and skin situations. However, it's important to make use of it as directed and observe good hygiene practices, such as washing clothes, bedding, and towels in hot water, to stop the spread of scabies and recurrence of the situation.
Scabies is extremely contagious, and it could unfold rapidly via shut physical contact. It is often acquired via skin-to-skin contact with an contaminated individual or by sharing bedding, towels, or clothes. The first symptoms of scabies typically appear inside a couple of weeks of initial exposure, and the commonest symptom is intense itching, particularly at night. Other symptoms could embody a rash, tiny blisters, or sores on the skin.
Eurax, also known by its generic name Crotamiton, is a topical medication commonly used for treating scabies and relieving itching. Scabies is a skin condition caused by tiny mites that burrow into the skin and lay eggs, inflicting intense itching and irritation.
Like all medications, Eurax comes with a threat of unwanted facet effects, though they aren't quite common. The most common unwanted side effects embody pores and skin irritation, redness, or a burning sensation on the utility site. In very rare circumstances, it could possibly trigger an allergic response, so it's important to discontinue use and seek medical consideration if any unexpected signs occur.
Eurax comes in a lotion or cream form and is applied to the complete physique, from the neck down, excluding the face. It is important to clean the medicine off after 24 hours and repeat the applying in seven days to make sure all the mites are killed. The medicine is not really helpful for use in children underneath three years old, pregnant or breastfeeding ladies, or people with recognized allergic reactions to any of its ingredients.
Eurax is assessed as a scabicidal and antipruritic medication, that means it kills scabies mites and relieves itchiness. It works by affecting the nervous system of the mites, paralyzing and killing them. It additionally has a neighborhood anesthetic impact, which helps to soothe the itchy pores and skin.
In contrast skin care routine for acne buy eurax toronto, the segmental graft requires no bench procedure and is usually placed extraperitoneally. Exocrine drainage is in to a Roux loop or obturated by duct injection with Neoprene. Nevertheless, as a result of much experimental work performed over the last two decades, the techniques of islet separation and preservation are much improved. The efficiency of current separation techniques is such that more than one donor is usually necessary for each islet cell transplant. Intraportal or intrasplenic injection appear to be the favoured sites of placement for islet grafts at present, but excellent islet survival has been reported in rodents following placement beneath the renal capsule. In addition to T- and B-cell-mediated immunological mechanisms, it is likely that scavenging mechanisms, such as phagocytosis by macrophages, assume an important role in islet graft destruction. Several hundred attempts at human islet cell grafting have been reported over the years, with insulin independence achieved for a few days only. However, a clinical programme of islet transplants using intraportal injection and achieving excellent insulin independence rates at up to 5 years has been reported recently by workers at Edmonton, Alberta. Highly efficient islet separation techniques, immediate transplantation of the prepared islets in to the portal vein by transhepatic or transjugular injection, and the use of the powerful immunosuppressive drugs tacrolimus and sirolimus have been the main factors underpinning this remarkable success. Allotransplantation of pancreas and duodenum along with the kidney in diabetic nephropathy. Results of segmental and pancreaticosplenic transplantation with pancreaticocystostomy. In most countries the demand for small-bowel transplantation to date has been low. In small children, transplantation of the liver together with the small bowel has produced better results than transplantation of the small bowel alone. The introduction in 1980 of ciclosporin A, a potent new non-steroidal immunosuppressant, sparked a second wave of worldwide enthusiasm, which has been sustained and has established heart transplantation as an extremely effective therapy for various types of end-stage heart disease. Indications 1 n Ischaemic heart disease and its complications, due to coronary n n 2 Lillehei was the first to report the technical feasibility of smallbowel transplantation in the dog. The introduction of ciclosporin A in 1978 revived interest in clinical small-bowel transplantation and this has been reinforced by the development of new agents such as tacrolimus and mycophenolate mofetil. Many major transplant centres now have modest series of small-bowel grafts, but graft survival longer than 3 years remains a rare event. Major clinical problems are: n Immunological rejection of the graft n Septicaemia due to bacteriological translocation across the graft during rejection episodes n Fluid and electrolyte losses from the graft n Graft-versus-host disease, which may be fatal n Technical problems, including vascular thrombosis and torsion of the graft pedicle. The physiological response of the small bowel of the dog to ischaemia including prolonged in vitro preservation of the bowel with successful replacement survival. Leave the posterior atrial wall with the orifices of the systemic and pulmonary veins intact. The wave of worldwide enthusiasm for 7 n On completion of the anastomoses, release the aortic clamp and 8 n When all air is displaced, clamp and remove the vent, release all allow the heart to fill via the coronary circulation, displacing air through the left ventricular vent. If the 6 Perform left and right atrial anastomoses, followed by aortic and pulmonary artery anastomoses, using continuous polypropylene sutures. Rejection Perform transjugular endomyocardial biopsies regularly initially every 35 days to detect and treat rejection as early as possible. Results One-year survival is 8590% in most large centres; 5-year survival is currently 75%. Further attempts were reported by Lillehei in 1969 and Barnard in 1971, with similar short-term survival. Reitz, working at Stanford, California, performed the first heart lung transplant under ciclosporin immunosuppression in 1981. Heartlung transplantation is now a well-established therapy for certain cardiopulmonary disorders. These results are the same for patients undergoing transplantation for cystic fibrosis and for the other indications. Whether heartlung transplantation will be succeeded by single or double lung transplants for cystic fibrosis and emphysema remains to be seen. The potentially serious disadvantage of heart-lung grafting for end-stage lung disease is that a healthy, well-functioning recipient heart is excised (and used for another heart recipient) to be replaced by an allograft that is susceptible to the many complications of allotransplantation, including the risk of both acute and chronic graft rejection. Long term follow-up after transplantation of insulin producing pancreatic islets in to patients with type I (insulin dependent) diabetes mellitus. Donor and recipient matching 1 n this is similar to that for heart transplantation. Size matching of the donor lungs to the recipient thoracic cage is very important, as over-inflation occurs if the lungs are relatively too small and inadequate ventilation occurs if the lungs are too large. Many potential donors are precluded on account of pulmonary infection due to mechanical ventilation. Thus, in view of size matching and scarcity of suitable uninfected donors, a 2 n Donor organs are much more difficult to obtain than hearts 433 27 Thorax E. Two Langenbeck retractors are used to expose the muscle and diathermy slowly through it layer by layer. Once through the latissimus, place a finger on the interspaces above and below the rib, and apply diathermy directly down to the rib. Pick up the anterior fascia with the cold tip of the diathermy, slide two fingers in to the space and apply diathermy on to the finger. The standard position is the 5th interspace (between the 5th and 6th ribs), corresponding to the line of the oblique fissure. Diathermy in a posterior to anterior direction through the intercostal muscles, to ensure that you stay on the superior border of the lower rib.
Cardiovascular progenitors are specified from mesodermal precursors shortly after gastrulation acne x lanvin eurax 20 gm order mastercard. Interestingly, these Isl1+ progenitors retain smooth muscle competency until late gestational stages. These observations lead to the speculation that the cardiac-smooth muscle bipotency of later Isl1+ cardiac progenitors may serve to form a smooth boundary between the heart chamber and great vessels at outflow and inflow tracts. Another population of the smooth muscle cells in the heart, the coronary wall, arises from the proepicardium, grape-like clusters that form between the sinus venosus and liver primordium. Using retroviral tagging methods, Mikawa and Gourdie demonstrated that the proepicardium is the source of the coronary vasculature (Mikawa and Gourdie 1996). Interestingly, these pro-epicardial progenitor cells are positive for several cardiac transcription factors including Isl1 and Nkx2-5. At later stage fetal hearts of 18 weeks of gestation, the relative and total numbers of Isl1+ cardiac progenitors were significantly reduced, consistent with rodent models (Bu et al. Thus, the lineage diversification of Isl1+ cardiac progenitors is evolutionally conserved in rodents and humans. While this system is highly useful for tracing the lineage contribution of specific cell types in mice, it does have limitations: (1) it inevitably turns the gradient of the expression level of the Cre driver gene in to a black-and-white image of the reporter gene, which potentially causes oversight of weak and short expression of the Cre drivers, (2) the readout depends on the ubiquity of the reporter gene and reporter, and (3) the recombination process causes a time gap between the expression of the endogenous gene and the reporter gene. These limitations can be critical when analyzing early embryonic events and sometimes complicate the interpretation of the results. Furthermore, the analyses of the same Isl1-Cre line with another reporter line, Gata4-flap reporter mice, in which alkaline phosphatase reporter cassette is knocked in to Gata4 locus, demonstrated robust expression of the reporter gene in the entire heart including the left ventricle and proepicardium (Ma et al. Importantly, these results raise the possibility that Rosa26-lacZ reporter line, the most commonly used reporter line, may not be a perfect standard for tracing the earliest events during embryogenesis. Obviously, a cell population should not be defined only by the expression of marker genes but also by its differentiation capability and behavior. Indeed, there is no evidence that these two populations are functionally different or mutually unexchangeable. The cardiac crescent is a dynamic structure to which the progenitors are continuously supplied from surrounding extra-crescent tissues. The identification of Isl1+ progenitors suggests that this supplementation continues throughout the process of heart tube formation, rightward looping, chamber ballooning and septation. Even at the late gestational stages, the addition of myocardia continues at specific domains of the venous pole. Thus, cardiogenesis is an even more dynamic process than was traditionally envisioned. In this regard, of great interest is the mechanism underlying the recruitment of cardiomyocytes from the yet-to-be committed progenitors at the later stages. Aside from its expression in the embryonic cardiovascular system, Isl1 is expressed in a variety of cell lineages including motor neurons and pancreatic endocrine islet cells. Hence, Isl1+ progenitors represent a pool of cells in various cardiac sub-lineages, which likely arise from a common source. The common function of the Isl1 transcription factor in these diverse populations is of interest. Isl1 expression strongly correlates with the cell cycle in the postnatal myocardium, such that Isl1 expression can be quickly turned on and off upon mitotic stimulation in the various sub-lineages of the cardiac progenitors (Nakano, unpublished). Therefore, Isl1 may well be regarded as a marker for mitotic cardiac progenitors/myocytes. Many signaling pathways are known to influence the differentiation and expansion of Isl1+ cardiac progenitors during development and cell culture. The precise analysis of the function of Isl1 transcription factor is a challenge as it is dependent on stage, sublineage, and expression dosage. The role of Isl1 in cardiac development Genetic analyses suggest a critical role of the Isl1 transcription factor during cardiogenesis. Mice that are homozygous null for Isl1 exhibit growth retardation at approximately E9. Atrial tissue in Isl1 mutants also showed a Cardiac Regeneration Using Isl1-positive Cardiac Progenitor Cells 193 significant reduction in size. Proliferative indices with BrdU labeling were significantly less in Isl1 mutants, with 76% reduction in splanchnic mesoderm and 39% reduction in pharyngeal endoderm relative to their controls where Isl1 is normally expressed. Isl1null cardiac progenitors underwent extensive apoptosis, whereas no apoptosis was seen in wild-type mice. This region includes several binding sites for forkhead (Fox) transcription factors, several members of which are expressed in the cardiogenic region during the early development in a highly conserved manner among humans, mice and chickens. These Fox transcription factors are implicated in early cardiac development (Papanicolaou et al. Mice lacking Mef2c are embryonic lethal with hypoplastic hearts and a single, linear ventricular chamber. During early avian cardiogenesis, canonical Wnt signals from the neuroectoderm inhibit the specification of cardiac progenitors, resulting in a crescent-shaped heart-forming region (Marvin et al. In vivo loss- and gain-of-function experiments using various Cre mice mostly resulted in the conclusion that Wnt/-catenin is involved in expansion of the cardiac progenitor population (Cohen et al. These data indicate that canonical Wnt signaling promotes the expansion of Isl1+ cardiac progenitors. The Wnt/-catenin pathway is clearly one of the most promising factors for cardiac regenerative purposes. These factors influence the expansion and differentiation of Isl1+ cardiac progenitors. In Isl1 null mice, the expression of Fgf10, Bmp4, and Bmp7 is severely down regulated or undetectable in pharyngeal endoderm and splanchnic mesoderm, and the domains expressing Fgf4, Fgf8, Bmp2, and Bmp6 are decreased in regions overlapping or contiguous with Isl1 expression (Cai et al.
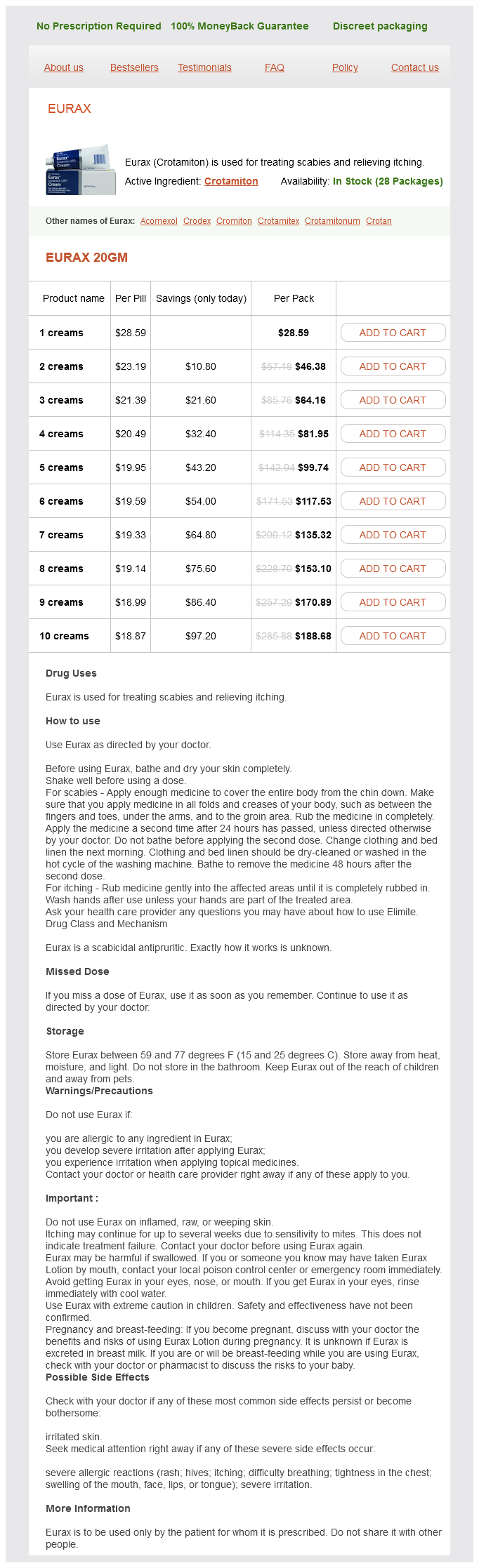
Eurax Dosage and Price
Eurax 20gm
- 1 creams - $28.59
- 2 creams - $46.38
- 3 creams - $64.16
- 4 creams - $81.95
- 5 creams - $99.74
- 6 creams - $117.53
- 7 creams - $135.32
- 8 creams - $153.10
- 9 creams - $170.89
- 10 creams - $188.68
If required skin care 1 20 gm eurax buy with visa, push the ureters caudally so that the uterine vessels can be clamped (see step 10). Continuous locked suture 11 n If the cervix is relatively long, clamp the paracervical tissue by ap- hysterectomy clamp. Divide the uterine vessels by cutting with a knife close to the clamp and around its tip and doubly ligate with a 1-synthetic absorbable suture. Postoperative If both ovaries have been removed discuss the use of hormone replacement therapy with the patient. Access 1 n Perform a bimanual examination under anaesthetic to decide on 2 n In general, if the uterus is mobile and it extends no further than the umbilicus, use a Pfannenstiel incision. Otherwise, use a lower midline incision, which may be extended around or even above the umbilicus if necessary. Complications n 2 n Ureteric 1 Reactionary or secondary haemorrhage from the vaginal angle may occur and presents as profuse vaginal bleeding. It can be dealt with through the vagina, applying a figure-of-eight suture to the bleeding points. Get expert urological assistance if there is any suggestion of such complications. Assess 1 n Plan the uterine incision(s): the aim is to remove as many fibroids through as few uterine incisions as possible. Try to avoid incisions in the posterior wall of the uterus, since these often give rise to bowel adhesions. Occasionally, if there are very dense pelvic adhesions and the uterus remains fixed deep in the pelvis, it may be difficult to remove the cervix. Proceed exactly as described, but there is no need to apply a clamp to the paracervical tissue (step 11). Action 1 n Unless removing a few subserous or pedunculated fibroids, bluntly fenestrate an avascular area of parametrium bilaterally. An alternative to rubber tourniquets to the ovarian vessels are ovarian artery clamps which can be placed medial to the ovaries, thereby avoiding ovarian ischaemia during surgery. To facilitate manipulating the fibroids, extend the cut in to each fibroid by about 1 cm. Fertility is improved only by the removal of submucous fibroids which substantially protrude in to the uterine cavity. If fibroids are multiple, the operation can be more time-consuming and hazardous than hysterectomy. The re- Prepare 1 n Bear in mind that this is the gynaecological operation with the 2 n Ensure the patient is aware that there is a risk of requiring hystergreatest expected blood loss, so optimize the haemoglobin concentration preoperatively. Several layers of sutures are needed to achieve an adequate repair and achieve haemostasis. If the endometrial cavity has been breached, repair this with a fine 2/0 absorbable suture. Most gynaecologists would not perform myomectomy on a patient who refuses blood products in an emergency. Adhere to the usual surgical principle of draining pus (sending some for culture), digitally breaking up loculi, irrigating the pelvis and abdomen (some use antiseptic wash-out) and inserting a drain through a separate abdominal incision. They arise in remnants of the mesonephric (Wolffian) duct and occasionally undergo torsion to produce acute abdominal pain. Distinguishing features are of recent sexual activity (which need not be "high-risk"), symmetrical lower abdominal pain, recent vaginal discharge and exquisite deep tenderness on bimanual examination. Take high-vaginal, intracervical and intracervical nucleic acid amplification swabs. These usually include a 2-week course of doxycycline to cover Chlamydia trachomatis, (the most common cause in the developed world), a single dose of ceftriaxone to treat gonorrhoea, and a 2-week course of either co-amoxiclav or metronidazole to cover anaerobes. The condition is almost always bilateral, although one tube may be more affected than the other. The tubes are oedematous and reddened, and pus is often seen dripping from the fimbrial end. If there has been little improvement in 3 n When involving the ovaries, endometriosis may be seen superfi- cally appears as small purple or dark-brown nodules, but appearances can be varied. Most women with the incidental finding of peritoneal endometriosis have no symptoms, and therefore require no treatment. If symptoms of abdominal pain, dysmenorrhoea and classically deep dyspareunia are present, ablate these areas of peritoneum with diathermy, taking extreme care not to injure vessels or the ureters deep to this tissue. Excise the cyst cavity, ensure haemostasis and repair the ovary with a fine polyglactin 910 suture if the cyst was large. In the large intestine it may produce sub-acute obstruction and can be extremely difficult to differentiate from carcinoma. Prepare 1 n Establish the haemoglobin concentration and group and save the patient. It may be wise to cross-match 4 units of blood preoperatively if blood is not immediately available, if the starting haemoglobin is low, or if blood loss is expected to be higher than usual for any reason. If a general anaesthetic is employed, a cuffed endotracheal tube is mandatory, to prevent aspiration of gastric contents, which are more liable to reflux in pregnancy. Once the head is delivered, displace the fetal head inferiorly, firmly but gently, to deliver the superior shoulder, and then displace the fetal head superiorly to deliver the posterior shoulder. Immediately after delivery of the baby, have the anaesthetist give an intravenous injection of synthetic oxytocin (Syntocinon) 10 units. Access 1 n A Pfannenstiel incision is suitable, but if you are inexperienced you may find a vertical sub-umbilical midline incision easier. The lower segment may be very thin, especially if the patient has been in labour for a long time, so take care not to cut too deeply and injure the neonate.