General Information about Escitalopram
The use of Escitalopram in treating melancholy and nervousness issues has been extensively studied and has been confirmed to be effective. In a research of over 1500 patients with melancholy, it was found that those who took Escitalopram had a considerably higher reduction in depressive symptoms in comparability with those who took a placebo. Similarly, in a study of patients with panic dysfunction, Escitalopram confirmed a significant decrease within the frequency and severity of panic attacks, as properly as total improvement in anxiety symptoms.
In conclusion, Escitalopram has confirmed to be an effective and well-tolerated therapy for melancholy and anxiousness disorders. Its selective motion on serotonin reuptake makes it a most popular selection for so much of sufferers. However, as with any medicine, it may be very important consult with a doctor and carefully monitor for any unwanted effects. With proper use and monitoring, Escitalopram may help improve the quality of life for these who suffer from these debilitating situations.
In addition to being effective in treating despair and anxiousness problems, Escitalopram has also shown promise in treating other circumstances such as obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), and premenstrual dysphoric disorder (PMDD). However, extra research is needed to determine its effectiveness in treating these circumstances.
Serotonin is a neurotransmitter that plays a crucial role in regulating our mood, sleep, urge for food, and overall well-being. It is also identified as the “happy hormone” as it is liable for making us feel good. However, in people with melancholy and anxiety issues, there might be an imbalance of serotonin within the mind, leading to signs similar to sadness, hopelessness, and anxiousness. Escitalopram works by blocking the reuptake of serotonin, permitting for extra of it to be obtainable in the brain, which in turn helps to enhance temper and cut back nervousness.
Escitalopram is often taken once a day and is out there in tablet form. The dosage may vary depending on the condition being handled and the patient’s response to the treatment. It is necessary to follow the prescribed dosage and not to abruptly stop taking it as it could result in withdrawal signs. Like other antidepressants, it could take several weeks for the full effects of Escitalopram to be felt. It is essential to seek the advice of with a doctor before starting or stopping this treatment.
Escitalopram is a selective serotonin reuptake inhibitor (SSRI), meaning that it targets solely the reuptake of serotonin and never other neurotransmitters like other antidepressants do. This selective action makes it a preferred and effective treatment for depression and anxiety disorders. Compared to other SSRIs, Escitalopram has a decrease chance of causing side effects such as weight acquire, sexual dysfunction, and fatigue, making it extra tolerable for sufferers.
As with any medicine, there are potential side effects of Escitalopram, together with nausea, dry mouth, dizziness, and headaches. In rare instances, it might additionally trigger extra severe unwanted aspect effects such as changes in heart rate and blood stress, in addition to serotonin syndrome, a probably life-threatening situation. It is important to monitor for any uncommon side effects and to debate them with a doctor.
Escitalopram, also identified by its model name Lexapro, is an antidepressant medication that is commonly prescribed for people who suffer from deep melancholy, panic problems, social anxiety issues, and other nervousness problems. Its mechanism of action is predicated on its ability to selectively block the reuptake of serotonin by the presynaptic membrane of the neurons in the mind. This in the end increases the serotonergic effect within the central nervous system, which is answerable for the development of the antidepressant impact and makes it highly efficient in treating panic and social anxiousness dysfunction.
The antigen is hydrolyzed to immunogenic small molecule antigen peptide by protein depression vs major depression buy escitalopram 10mg visa. As the pathogenesis of inflammatory myopathy, innate immunity has been recognized by more and more scientists, and its specific process still needs to be further explored [59]. In addition, some muscle cells and endothelial cells can also produce cytokines and participate in the inflammatory response. The pathogen of chronic infection can activate the immune response of people with autoimmune tendency, and it is more likely to cause autoimmune diseases. Avoiding microbial infection may delay the development of the disease and reduce the rate of hospitalization and mortality. Drug-induced myositis has been reported in early years, such as penicillin, whose decomposition product penicillamine can be used as a hapten to affect the stability of the autoimmune system and its tolerance to autoantigens. Muscle biopsy shows the characteristics of necrotizing myopathy, and the symptoms of such drugs are not relieved. Some scientists believed that statins mediate the occurrence of inflammatory myopathy by inducing the production of autoantibodies, but the specific mechanism is not clear. In addition, other drugs such as zidovudine, carbazide, and zoledronic acid have been reported to induce myopathy. Therefore, in clinical work, it should be alert to the occurrence of drug-induced myositis [70, 71]. The repair of skeletal muscle injury has been a longterm concern and research basic problem in the sports medicine field. Many researchers have carried out many studies from different angles, but many mechanism problems have not been completely solved. The latest research found that the early inflammatory reaction after skeletal muscle injury plays an important role in the repair of muscle besides the traditional phagocytosis. It was also found that, in addition to inflammatory cells, skeletal muscle cells can also secrete the aforementioned cytokines, which may coordinate with each other in skeletal muscle injury and repair, and play a role in myogenic regulation [7274]. Clinically, it is named as different diseases due to different degree and location of degeneration: deformity spondylosis, osteoarthritis of spine, instability of lumbar spine, protrusion of intervertebral disc, degenerative spondylolisthesis, degenerative stenosis of spinal canal, ossification of ligament (posterior longitudinal ligament and ligamentum flavum), and so on [75]. With the increase of age, the disc began to degenerate, the water content of the nucleus pulposus in the disc decreased, and the strength and toughness of the peripheral fiber ring affected by the external force decreased, resulting in the decrease of the elasticity and antiload effect of the disc. At this time, in daily life, the repeated compression, flexion, and torsion of lumbar and cervical intervertebral disc will further aggravate the disc herniation and compress the nerve root, resulting in neck, shoulder, and leg pain. Spinal degenerative disease is the main disease that causes neck and low back pain, and it is also a common orthopedic disease, accounting for about 1/3 of orthopedic outpatient. In the early stage, conservative treatment such as medicine, traction, massage, and physical therapy are mainly advocated. For those who have no effect on long-term conservative treatment (more than 6 months), surgery is generally considered. The biochemical mechanism of degenerative change is generally believed to be closely related to the metabolic disorders of three chemical components: proteoglycan complex, collagen fiber, and elastin. In addition, chondroblast deficiency and soft tissue deficiency can aggravate the degeneration of bone and joint. Although the age is the same, the degree and scope of degeneration are also different, mainly depending on the following factors. The age of degeneration can be advanced by overload, for example, athletes in some sports and workers whose spine has been pressed for a long time. If the average pressure is more than 350 kg for a long time, the fiber ring will expand from the center to the surrounding or even break (Table 1). The pressure load of the third lumbar intervertebral disc is about 70 kg in the upright position of the human body in the poor posture and 120 kg if the lumbar spine is flexing forward. In this case the pressure in the disc can be increased to 340 kg with another 20-kg load. Thus it can be seen that the change of posture is of great significance for spinal degeneration. Some chronic strain and some occupations make the spine in vibration state for a long time and make the intervertebral disc suffer from repeated high-pressure impact and suffer from chronic injury. At the same time, it can also make nucleus pulposus and annulus fibrosus that cause pressure on the surrounding ligaments, resulting in fracture and subperiosteal hemorrhage, and in serious cases, it can cause nucleus pulposus to protrude. Variable Total patients Sociodemographics Age Mean 2029 years 3039 years 4049 years 5059 years Gender Female Male Body mass index Normal (1824. All kinds of violence can cause the injury of bone joint, tendon, and ligament and accelerate the process of local degeneration. In addition, repeated spinal puncture, heavy traction, and irregular massage will damage the spine structure and accelerate the degeneration. Chronic inflammation of various kinds of inflammation around the spine can directly or indirectly stimulate the surrounding muscles, ligaments, and bone joints, resulting in changes in the stability of the spine and aggravating the process of degeneration [7779]. The lateral recess is bordered laterally by a pedicle, dorsally by a superior articular facet, and ventrally by a vertebral body and discs. The foraminal space is bordered by cephalad and caudal pedicles and facet joints dorsally and a vertebral body and discs ventrally. After the surface of vertebrae was damaged, the periosteal hematoma was formed; the fibroblasts began to be active and gradually grew into the hematoma, gradually replacing the hematoma with granulation tissue. If stimulation is repeated, new and old lesions may coexist in the same vertebral segment.
Desvenlafaxine for the treatment of vasomotor symptoms associated with menopause: a double-blind depression definition in history order escitalopram overnight, randomized, placebo-controlled trial of efficacy and safety. Treatment of vasomotor symptoms of menopause with black cohosh, multibotanicals, soy, hormone therapy, or placebo: a randomized trial. Behavioral weight loss for the management of menopausal hot flashes: a pilot study. Exercise training reduces the acute physiological severity of post-menopausal hot flushes. Yoga and meditation for menopausal symptoms in breast cancer survivors a randomized controlled trial. Effects of stellate ganglion block on vasomotor symptoms: findings from a randomized controlled clinical trial in postmenopausal women. Neurokinin 3 receptor antagonism as a novel treatment for menopausal hot flushes: a phase 2, randomised, double-blind, placebo-controlled trial. Other terms frequently employed to describe this sector include complementary, holistic, folk, traditional, natural or integrative (integrated) therapies/ medicine. They point out that conventional medicine is today more effective than it ever has been, and that turning to uncertain alternatives is therefore less than rational. We have attempted to answer this question by conducting a systematic review of all 73 surveys that addressed 264 Alternative Therapies for the Management of Menopausal Symptoms 265 this issue [2]. Many seem to promote unproven or disproven treatments and some even discourage the use of proven conventional therapies. There was very little consensus amongst the seven authors as to which treatments were recommendable, and the vast majority of the recommended therapies were not supported by sound evidence [3]. Similarly, regular fibre intake seemed to be effective in reducing serum total cholesterol in hypercholesterolemic postmenopausal women. Black cohosh seemed to be effective therapy for relieving menopausal symptoms, primarily hot flashes, in early menopause. Phytoestrogens, including isoflavones and lignans, appeared to have only minimal effect on hot flashes but may have other positive health effects. Promising evidence also existed for the effectiveness of vitamin K, 266 Alternative Therapies for the Management of Menopausal Symptoms a combination of calcium and vitamin D as well as for a combination of walking combined with other weight-bearing exercise in reducing bone mineral density loss and the incidence of osteoporosis/fractures in postmenopausal women [6, 7]. In premenopausal women, encouraging evidence for the effectiveness of vitamin B6 supplementation has been found [8]. Similarly, there is insufficient evidence for the effectiveness of other popular modalities such as yoga [4] or ginseng [9]. In particular, oral supplements can cause adverse effects through · the toxicity of an ingredient · Interactions with prescribed medications · Contamination · Adulteration Alternative therapies and therapists are usually not tightly regulated, which can increase their risks considerably. The most obvious of those is that a curable condition might get treated for prolonged periods of time with a therapy that is ineffective. This may well be true, but it is fairly irrelevant for judging the value of any given intervention. Therapeutic decisions should never be guided by their effectiveness or their safety in isolation but by balancing the two factors. Oral dietary supplements, including herbal remedies, for instance, can and should be tested much like conventional medicines, i. When it comes to other treatments, such as yoga, hypnotherapy or acupuncture, things can get more complex. What, for example, might be a reasonable placebo control for a trial of hypnotherapy In some instances, this might mean that placebo controls and patientblinding are simply impossible. In our experience, the biggest problem lies in the mindset of alternative therapists who often are reluctant to conduct rigorous tests of their interventions. Whether this sentiment originates from the fear that such tests might be negative or from a wider antiscientific attitude seems irrelevant; the fact is that it represents an important obstacle to progress in this area. Belief can be wrong, practice can be misguided and popularity is certainly not a reliable indicator for effectiveness. The history of medicine is littered with examples which demonstrate how misleading these fallacies can be. This conclusion seems obvious to patients and therapists alike yet it is fallacious. Apart from the treatment per se, a whole range of factors can cause or at least contribute to a clinical improvement in that patient: the placebo effect, the natural history of menopause, the regression towards the mean, to mention just three. A long tradition of use can, of course, be an indicator for the safety and efficacy of a treatment, but it can never be a proof. On the contrary, a long history might also mean that the origins of that therapy reach back to a time when our understanding of anatomy, physiology etc. This, in turn, might lessen the chances for any such intervention to be plausible or effective. The implication is that conventional treatments are unnatural, heavily based on chemicals which are potentially harmful. Great expectations: what do patients using complementary and alternative medicine hope for The Desktop Guide to Complementary and Alternative Medicine: An Evidence-Based Approach. Effects of herbal and dietary supplements on cognition in menopause: a systematic review. Natural health products in the prevention and treatment of osteoporosis: systematic review of randomized controlled trials. Effect of weighted exercises on bone mineral density in post menopausal women: a systematic review. Ginseng for managing menopause symptoms: a systematic review of randomized clinical trials.
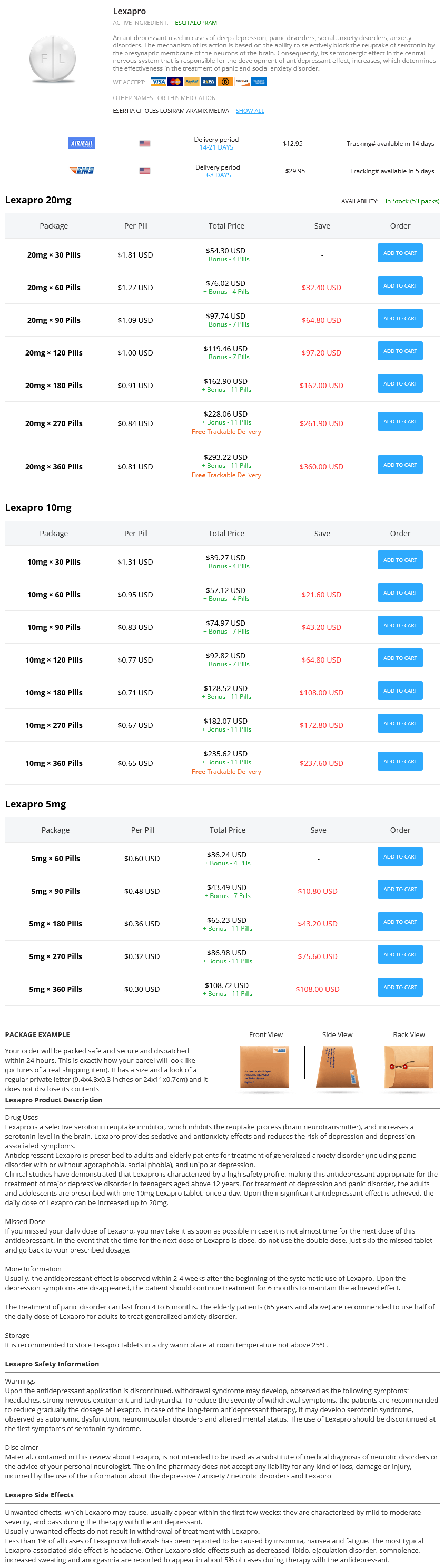
Escitalopram Dosage and Price
Lexapro 20mg
- 30 pills - $54.30
- 60 pills - $76.02
- 90 pills - $97.74
- 120 pills - $119.46
- 180 pills - $162.90
- 270 pills - $228.06
- 360 pills - $293.22
Lexapro 10mg
- 30 pills - $39.27
- 60 pills - $57.12
- 90 pills - $74.97
- 120 pills - $92.82
- 180 pills - $128.52
- 270 pills - $182.07
- 360 pills - $235.62
Lexapro 5mg
- 60 pills - $36.24
- 90 pills - $43.49
- 180 pills - $65.23
- 270 pills - $86.98
- 360 pills - $108.72
This method divides the body into body surface areas of 9% (the head anxiety buzzfeed 10mg escitalopram amex, each upper limb, the front of the trunk, the back of the trunk, the front of each lower extremity, and the back of each lower extremity). Computerized methods have evolved and demonstrate high correlation and reproducibility. Second-degree burns are further categorized into superficial and deep partial thickness burns. A superficial partial thickness burn extends into the superficial papillary dermis and appears red in color with significant weeping and blisters. The Lund-Browder burn diagram and table indicate the varying proportions in surface area in persons with different ages. A careful burn diagram should be completed at the time of initial evaluation, including wound size, location, and estimated burn depth. The Lund-Browder chart should be used in pediatric patients because the body surface area relationships vary with age. Later, when insulin resistance and associated hyperglycemia develops, glucose infusions should be modulated. Colloids have the potential to increase oncotic pressure and thereby reduce fluid shifts and losses. Controversy remains as to the ideal time for initiation of colloid therapy in burn resuscitation. There is a general trend now to initiate colloids earlier than the previously recommended time of 24 hours. The reasons for using hourly urine output are that it is easily measured (once a Foley catheter has been placed), it reflects glomerular filtration rate and renal blood flow, and it is a surrogate for endorgan perfusion and an indirect correlate of cardiac output. When assessing circulation 18 hours after the injury, these central variables of cardiac filling and function will normalize with this resuscitation strategy. First, the skin, which in burn injury is the damaged organ, has a very high density of 1 adrenoceptors in its vascular bed and secondly, this compartment receives a significant portion of the fluid volume provided by resuscitation, thereby significantly increasing the risk of progression of the burn wound from second- to third-degree injury. There is scientific evidence in humans that support skin ischemia in edematous tissue after fluid resuscitation and this may be assumed to be a significant risk for deepening of the burn wound. Signs of resuscitation failure include low urine output, repeated episodes of hypotension or need for vasopressors, worsening of base deficit, or fluid infusion in excess of predicted resuscitation needs in the first 24 hours. Hemodynamic monitoring modalities to obtain this information on cardiac function include transthoracic and/ or transesophageal echocardiography, measures of cardiac preload or fluid responsiveness. The major limitation of routinely using these measures for all resuscitations is that they have not been validated as resuscitative endpoints in the burn injury population; targeting multiple endpoints may result in excess fluid administration. With large volume resuscitation, monitoring of abdominal, ocular, and extremity-fascial compartments for hypertension should regularly be performed. The most commonly used method to monitor intraabdominal pressure is measurement of intravesical pressure through a catheter inserted in the urinary bladder. Values above 25 mm Hg generally necessitate intervention, whereas values between 12 and 25 mm Hg indicate the need for close observation for targets of initial resuscitation in burn injury patients remain largely unknown. While traditional markers such as blood pressure, urinary output, and cardiac output are helpful, they do not sufficiently reflect the adequacy of regional perfusion and microcirculation. Even when macrocirculatory variables are within therapeutic goals, signs of tissue hypoperfusion may persist. This experience has confirmed earlier studies showing that cardiac output and other parameters require 18 to 24 hours to normalize following burn injury no matter what resuscitation strategy is employed. Hence leaky lungs from inhalation injury and during ventilationperfusion abnormalities it may give incorrect estimates of 87 · Acute and Anesthetic Care of the Burn-Injured Patient 2757 evaluation. It should also be suspected not only in patients with major burns but particularly in those who have received an amount of fluid resuscitation well beyond that predicted based on weight and burn size. Strategies to limit fluid creep may include albumin administration during early resuscitation and, more commonly, initiation of "colloid rescue" early (12-24 hours) after the burn injury when capillary integrity is thought to be restored. Hypertonic saline may also be beneficial in limiting fluid volumes, but careful monitoring is needed, as hypernatremia is associated with the development of acute renal failure. High-voltage injury is characterized as more than 1000 V, and leads to damage that extends into the surrounding tissues, particularly to muscle around long bones. Exposure to current generated may also cause cutaneous injury by transformation of electrical energy to thermal energy. Burns due to lightning are common but typically quite superficial because of the short duration of contact between the energy source and the victim. Evaluation for associated traumatic injury, particularly to the spinal cord, should take place, including assessment for event-associated blunt thoracic or abdominal trauma. In high-voltage electrical injuries, urgent surgery may be life-saving, and is necessary to allow the highest chance for limb salvage. After initial burn wound excision, further debridement may be indicated to ensure adequacy of excision of necrotic tissue before reconstruction. Wound management of high-voltage injuries often requires staged debridement, because the extent of myonecrosis is often difficult to initially ascertain and myonecrosis can extend over time. High-voltage electrical injuries can be severe resulting in the need for amputations. The tetanic contraction of muscle caused by continued electrical stimulation may cause bone damage including vertebral fractures. Electrical injury affects the cardiovascular system by directly causing necrosis of the cardiac muscle and by inciting dysrhythmias. Cardiac standstill and ventricular fibrillation are the most serious cardiac complications of electrical injury. Patients without electrocardiographic changes on presentation are unlikely to experience life-threatening arrhythmias. Enzyme markers of cardiac injury may be misleading, as normal enzyme concentrations in the circulating blood do not exclude the possibly of a conduction system injury with consequent rhythm disturbances.