General Information about Dapoxetine
Dapoxetine, additionally known by its brand name Priligy, is a medicine commonly prescribed for the treatment of untimely ejaculation (PE). Premature ejaculation, also referred to as rapid or early ejaculation, is a standard sexual dysfunction affecting many males. It is characterized by the shortcoming to control or delay ejaculation throughout sexual exercise, resulting in misery and frustration for each the individual and their partner.
Dapoxetine was initially developed as an antidepressant, however its effectiveness in delaying ejaculation was discovered during medical trials. It was subsequently approved by the US Food and Drug Administration (FDA) in 2004 as the first medication particularly designed for the therapy of premature ejaculation. Since then, it has turn into a popular choice amongst males in search of assist for this condition.
In addition to its fast-acting nature, dapoxetine has been proven to be effective in delaying ejaculation. Several scientific trials have shown that men who took dapoxetine skilled a significant enhance in the time to ejaculation in comparability with those that took a placebo. It has additionally been found to enhance total sexual satisfaction and scale back distress related to untimely ejaculation.
The precise causes of premature ejaculation are not fully understood. It can be each psychological and physical in nature. Psychological factors corresponding to nervousness, stress, and relationship issues can contribute to the problem. Physical causes may include hormonal imbalances, irritation of the prostate, or unwanted aspect effects from sure medicines.
In conclusion, dapoxetine has revolutionized the remedy of premature ejaculation and has provided a much-needed choice for males fighting this situation. Its fast-acting nature, effectiveness, and safety profile make it a preferred alternative among both sufferers and healthcare providers. However, it could be very important do not neglect that untimely ejaculation can have varied underlying causes and that a comprehensive treatment approach could additionally be necessary for long-term success.
Dapoxetine works by inhibiting the reuptake of serotonin, a neurotransmitter concerned in regulating temper and emotions. Serotonin also performs a role in controlling the timing of ejaculation. By blocking the reuptake of serotonin, dapoxetine helps to increase the extent of this chemical in the brain, which in turn delays ejaculation.
While dapoxetine has been proven to be effective in treating premature ejaculation, it isn't a treatment for the situation. It is essential to handle any underlying psychological or bodily components contributing to the problem in addition to taking treatment. Counseling, therapy, and/or behavioral strategies could also be beneficial together with dapoxetine to help improve sexual perform.
Dapoxetine is usually well-tolerated, with few unwanted effects reported. The most common ones include nausea, headache, dizziness, and diarrhea. These side effects are usually delicate and momentary, and tend to improve with continued use of the medicine. As with any treatment, it is important to focus on potential dangers and advantages with a healthcare professional earlier than starting therapy.
One of the primary benefits of dapoxetine is its fast onset of action. It can be taken on an as-needed basis, approximately 1-3 hours prior to sexual activity, and its effects can final for several hours. This makes it a handy possibility for males who don't want to take a every day medication.
A study of needle angles in volunteers undergoing magnetic resonance imaging impotence vasectomy generic dapoxetine 30 mg with amex, Anesthesiology 105:9, 2006. Serlo W, Haapanemi L: Regional anaesthesia in paediatric surgery, Acta Anaesthesiol Scand 29:283, 1985. Casati A, Danelli G, Baciarello M, Corradi M, et al: A prospective, randomized comparison between ultrasound and nerve stimulation guidance for multiple injection axillary brachial plexus block, Anesthesiology 106:992, 2007. Ababou A, Marzouk N, Mosadiq A, Sbihi A: the effects of arm position on onset and duration of axillary brachial plexus block, Anesth Analg 104:980, 2007. Bier A: Ueber einen neuen weg lokalanasthesie an den gliedmassen zu erzcugen, Verh Dtsch Ges Chir 27:204, 1908. Marhofer P, Nasel C, Sitzwohl C, Kapral S: Magnetic resonance imaging of the distribution of local anesthetic during the threein-one block, Anesth Analg 90:119, 2000. Lopez S, Gros T, Bernard N, Plasse C, et al: Fascia iliaca compartment block for femoral bone fractures in prehospital care, Reg Anesth Pain Med 28:203, 2003. Valade N, Ripart J, Nouvellon E, Cuvillon P, et al: Does sciatic parasacral injection spread to the obturator nerve Gaertner E, Lascurain P, Venet C, Maschino X, et al: Continuous parasacral sciatic block: a radiographic study, Anesth Analg 98:831, 2004. Ichiyanagi K: Sciatic nerve block: lateral approach with the patient supine, Anesthesiology 20:601, 1959. Fanelli G, Casati A, Garancini P, Torri G: Nerve stimulator and multiple injection technique for upper and lower limb blockade: failure rate, patient acceptance, and neurologic complications. Paqueron X, Bouaziz H, Macalou D, Labaille T, et al: the lateral approach to the sciatic nerve at the popliteal fossa: one or two injections Arcioni R, Palmisani S, Della Rocca M, Romano S, et al: Lateral popliteal sciatic nerve block: a single injection targeting the tibial branch of the sciatic nerve is as effective as a double-injection technique, Acta Anesthesiol Scand 51:115, 2007. Capdevila X, Biboulet P, Morau D, Bernard N, et al: Continuous three-in-one block for postoperative pain after lower limb orthopedic surgery: where do the catheters go Capdevila X, Pirat P, Bringuier S, Gaertner E, et al: Continuous peripheral nerve blocks in hospital wards after orthopedic surgery: a multicenter prospective analysis of the quality of postoperative analgesia and complications in 1,416 patients, Anesthesiology 103:1035, 2005. Auroy Y, Narchi P, Messiah A, Litt L, et al: Serious complications related to regional anesthesia: results of a prospective survey in France, Anesthesiology 87:479, 1997. Reiestad F: Interpleural catheter in the management of postoperative pain, Reg Anesth 11:89, 1986. Mehta Y, Swaminathan M, Mishra Y, Trehan N: A comparative evaluation of intrapleural and thoracic epidural analgesia for postoperative pain relief after minimally invasive direct coronary artery bypass surgery, J Cardiothorac Vasc Anesth 12:162, 1998. Lancaster P, Chadwick M: Liver trauma secondary to ultrasoundguided transversus abdominis plane block, Br J Anaesth 104:509, 2010. Farooq M, Carey M: A case of liver trauma with a blunt regional anesthesia needle while performing transversus abdominis plane block, Reg Anesth Pain Med 33:274, 2008. Chayden D, Nathan H, Chayen M: the psoas compartment block, Anesthesiology 45:95, 1976. Capdevila X, Coimbra C, Choquet O: Approaches to the lumbar plexus: success, risks, and outcome, Reg Anesth Pain Med 30:150, 2005. Danelli G, Ghisi D, Bellinghieri F, Borghi B, et al: the nerve stimulation technique versus the loss of resistance technique for the posterior approach to lumbar plexus block: a randomized, prospective, observer-blinded, pilot study, Minerva Anestesiologica 77:959, 2011. Capdevila X, Macaire P, Dadure C, Choquet O, et al: Continuous psoas compartment block for postoperative analgesia after total hip arthroplasty: new landmarks, technical guidelines, and clinical evaluation [see comment], Anesth Analg 94:1606, 2002. Auroy Y, Benhamou D, Bargues L, Ecoffey C, et al: Major complications of regional anesthesia in france: the sos regional anesthesia hotline service, Anesthesiology 97:1274, 2002. Ultrasound imaging can elucidate the structure of peripheral nerves and adjacent anatomic structures for regional block. Anatomic variation in nerve position and course, which is a potential source of block failure, can be directly visualized. Successful local anesthetic injections clarify the border of the nerve and track along the nerve path and its branches. Ultrasound imaging allows direct visualization of peripheral nerves, the block needle tip, and local anesthetic distribution. This chapter describes the general principles of ultrasound imaging for regional blocks and gives specific examples of peripheral nerve block procedures. High-frequency ultrasound beams are well collimated and therefore can provide high resolution. For most regional blocks, the highest frequency is selected that adequately penetrates the depth of field. Sound waves reflected at the interface of two tissues with different acoustic impedances generate echoes. Ambient lighting has a large effect on visual discrimination; therefore, dim lighting without glare is especially useful for imaging low-contrast targets such as peripheral nerves. Local heterogeneities in soft tissue can cause artifactual bending of the block needle on ultrasound scans, the so-called bayonet artifact5,6. Bayonet artifacts are commonly observed during the lateral in-plane approach to popliteal block (see "Sciatic Nerve Blocks in the Popliteal Fossa") because more adipose tissue is present over the nerves near the posterior midline of the leg. When this does not occur, reverberation artifacts are displayed deep to the reflector. Reverberation artifacts are commonly observed from the block needle shaft at shallow angles of insertion because sound waves bounce back and forth between the walls of the needle before returning to the transducer. Comet tail artifact is another type of reverberation artifact and helps identify strong reflectors such as the pleura during supraclavicular and intercostal blocks. At low receiver gain, the comet tail is seen as a tapering series of discrete echo bands just deep to a strongly reflecting structure. The spacing between the bands represents the distance between the anterior and posterior walls of the object. Comet-tail artifact 1752 Chapter 58: Ultrasound Guidance for Regional Anesthesia 1753 from the pleura relates to lung water content, because small collections of lung water lined by the strongly reflecting pleura can allow the sound beam to enter and then return at varying times to the transducer. Third, all reflectors are assumed to be on the central ray of the transducer beam. When this assumption is not true, out-of-plane artifacts are observed (slice thickness artifacts). Definitive proof of out-of-plane artifacts requires multiple views, which are recommended when such ambiguities arise.
Just as the senses have limitations and can be "fooled" under certain circumstances impotence reasons 60 mg dapoxetine overnight delivery. Intelligent users of these devices must understand their basic design assumptions to predict when they are likely to produce erroneous data. Comparing a measurement with the gold standard of that measure usually determines an error. Unfortunately, all measurements, even the so-called gold standards are subject to errors with respect to reproducibility. For example, arterial blood pressure can be measured in several ways, ranging from listening to Korotkoff sounds by the use of a sphygmomanometer cuff and stethoscope to continuous measurement via an intraarterial cannula. Unfortunately, each of these techniques provides slightly different arterial blood pressure values and different sources of error. The choice of method may be determined by accuracy or by the need for the frequency of the data and the ease of retrieving these data. An automatic oscillometric device is usually chosen over manual auscultatory measurements for ease of acquisition and reproducibility. Two people taking auscultatory blood pressure measurements may hear the Korotkoff sounds at slightly different points and record different arterial blood pressures. The smallest change in the measured variable that could affect a clinical decision determines the required accuracy of a clinical monitor. Consider a theoretic device that estimates hemoglobin (Hb) concentration by measuring in vivo light absorbance. This Hb concentration measured by absorbance (SpHb) of the finger is compared with the total Hb (tHb) concentration determined from in vitro laboratory analysis. SpHb is significantly dependent on the perfusion (temperature) of the finger (see Chapter 61). Yet, tHb can be associated with errors with arterial blood sampling and in vitro analysis of the sample by any method. Nevertheless, in vitro laboratory analysis is considered to be the gold standard in this comparison of methods. The SpHb value can be compared with that of the tHb by the determination of bias and precision as recommended by Bland and Altman1. Bias is the average difference between simultaneous values from the two methods, termed the systematic error or offset. If the SpHb reads an average of 5 g/dL higher than the tHb, then it has a bias of 5 g/dL and we can adjust for that systematic error by recalibrating the device. Precision is the standard deviation of the difference between the two measurements, and it quantifies the random error or scatter. We can adjust for systematic error (bias) by recalibration, but no method exists to adjust for a random error. Both the bias and the precision may vary over the range of values of clinical interest. A monitor may give accurate and precise values in the normal range but have a bias or precision error at the very range we are interested in to make a clinical decision. For example, a Hb measurement device may accurately read Hb values from 11 to 14 g/dL but have significant errors with values less than 11 g/dL (see Chapter 61), which is the range most clinically important. Such a monitor may pass initial scrutiny but be clinically useless or harmful by inducing us to initiate or withhold treatment based on poor information. The bias plot is a way to compare two different methods of measuring the same variable. Examples are plotted on the right for hemoglobin (Hb) values, blood analysis versus Hb absorbance. It is a plot of the difference between the two measurements being compared versus the average of those two measurements. A, If one method constantly measures slightly higher than the other by a consistent value, then the method has a positive bias. If it has only a slight variation around that bias, then the method is said to have low random error or precision, which equals the standard deviation of the differences. B, the values are randomly scattered, such that the average difference is near zero, but the precision value is large. This large random error makes the device unusable because calibration will not improve this random error. C, this is the optimal device, in that it has a bias near zero and a small precision. D, this device has reasonable precision at any given value, but the bias varies, depending on the value, leading to a useless device with undefined accuracy and precision over the clinical range necessary. A dimension is a specific category or type of physical quantity; for example, mass, length, time, energy, or any of their derivatives. Examples of units include the meter (length), second (time), kilogram (mass), ampere (current), and degree Kelvin (temperature). A 30° day in Fahrenheit is literally freezing; a 30° day in Celsius is rather hot. The force of gravity on the unknown mass of fruit is balanced by the known standard masses on the opposite side of the balance. A Wheatstone bridge is an electronic circuit designed to enable an unknown resistance to be calculated by knowing two sets of variables: (1) the voltage drop across the bridge, and (2) the other resistances in the circuit (see Appendix 44-3). In this case, the downward pressure of the fluid, as determined by its density and height, balances the upward pressure of the central venous system, caused by hydrostatic and elastic recoil forces. In the absolute sense, usually reserved for thermonuclear weapons, atomic reactors, and the sun, matter can be converted into energy and vice versa (Table 44-1). When we measure the central venous pressure using a simple manometer, we are observing the balance of forces between the venous pressure and the force of gravity acting upon a fluid column. When the same pressure is electronically measured, we are balancing a Wheatstone bridge (a system of resistors used to determine an unknown resistance).
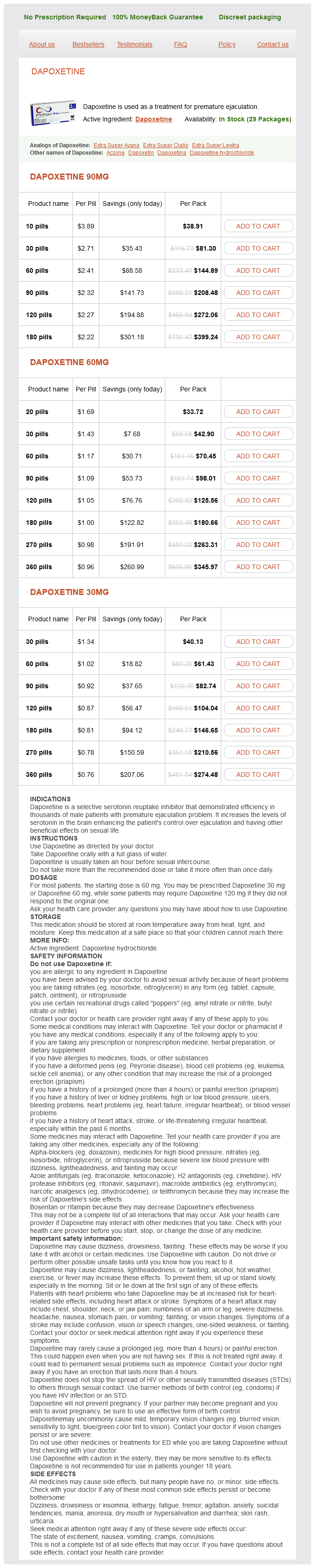
Dapoxetine Dosage and Price
Dapoxetine 90mg
- 10 pills - $38.91
- 30 pills - $81.30
- 60 pills - $144.89
- 90 pills - $208.48
- 120 pills - $272.06
- 180 pills - $399.24
Dapoxetine 60mg
- 20 pills - $33.72
- 30 pills - $42.90
- 60 pills - $70.45
- 90 pills - $98.01
- 120 pills - $125.56
- 180 pills - $180.66
- 270 pills - $263.31
- 360 pills - $345.97
Dapoxetine 30mg
- 30 pills - $40.13
- 60 pills - $61.43
- 90 pills - $82.74
- 120 pills - $104.04
- 180 pills - $146.65
- 270 pills - $210.56
- 360 pills - $274.48
The capacitance of the skin (Cs) also acts to attenuate the low-frequency components and distort the waveform erectile dysfunction what age does it start purchase 90 mg dapoxetine free shipping. Skin resistance, which may be a megaohm (106 ohms) for dry skin, can be reduced to a few hundred ohms by conductive gels. Although the electrical current in metals consists entirely of electron flow, both positive and negative ions migrate in tissues. Negative ions tend to accumulate at the positive electrode (the anode), and positive ions accumulate at the negative electrode (the cathode). The current therefore decreases and the effective impedance between the electrodes increases. Such attenuation could be misinterpreted as a lack of electrical activity and result in inappropriate administration of a second shock. A partial solution to the problem is the use of a nonpolarizable electrode, such as a silver and silver chloride combination. Stereo speakers use resistors to act as an impedance to high-frequency components of sound, allowing only the bass frequencies to pass to the woofer speaker. Capacitors are used as a high-pass filter to allow only the high frequencies to get to the tweeter speaker. For rapid interpretation and diagnosis, the amplitude versus time data are usually transformed into plots of amplitude (or power) versus frequency. This motor nerve then conducts the impulse to the muscle, where a twitch is generated. We can understand the in-use failings of this device by following the path of the signal. If the coupling of the electrodes to the patient is poor, that is, if the electrodes are dry or good skin contact is not made, then the circuit will have high resistance and little current will flow (see earlier discussion on direct current and equation 2), resulting in a diminished twitch. In summary, the simplest way to be certain that this monitor is properly functioning is to perform both a positive control (see the desired response of the thumb twitch before the chosen drug is administered) and a negative control (see the twitch disappear in response to administered drug) (see Chapters 49 and 53). Evoked-potential (evoked-response) monitors can determine the status of multiple parts of the sensory nervous system by measuring the central nervous system response to a discrete sensory stimulus. The amplitude of the evoked response measured at the skin can be small-less than 1 V in the case of acoustic cortical potentials. Rather than trying to measure the small response to a single stimulus, we average the responses from hundreds (or thousands) of stimuli. Chapter 44: Fundamental Principles of Monitoring Instrumentation 1331 Because we seek the evoked responses that consistently occur at the same time after the known stimulus, this averaging process reinforces the signal from the evoked response, and the random noise tends to cancel itself. In this way, we commonly measure signals whose amplitude is approximately 1% the amplitude of the background noise. Whenever charged particles are moving, a magnetic field is generated in a direction perpendicular to the motion. Paramagnetism is a form of magnetism exhibited only in specific substances in the presence of an external magnetic field. This property is used to measure both inspired and expired oxygen concentrations; chemical methods similar to fuel cell amperometric sensors and polarographic electrodes are too slow to respond. In a fast-responding paramagnetic oxygen sensor, 100% oxygen can exert a pressure of 3 Pa in a 2. Visible light and infrared light demonstrate several properties common to all electromagnetic radiation. Light represents a form of energy that, when passing through matter, may be reflected, transmitted, or absorbed. Although light itself cannot be stored, it can be converted into some other form of energy such as electricity, chemical energy, and heat. In addition, light can be generated from other forms of energy, including heat (incandescent), electrical (gas discharge), and chemical (photoluminescent) energy. Every substance with a temperature above absolute zero emits electromagnetic radiation, called black body radiation. This radiation is characterized by a frequency and wavelength that are related by the speed of light: frequency = speed of light ÷ wave length (c = speed of light = 3 × 108 m/sec or 186,400 miles/sec or 7. High energies or temperatures are associated with high frequencies and short wavelengths, such as those of gamma rays and x-rays. As wavelength increases to the micron range, ultraviolet radiation proceeds to visible light (approximately 0. The particles in motion in sound waves are in the same direction as the propagation (longitudinal waves), whereas in electromagnetic waves, the electric and magnetic fields are perpendicular to the direction of propagation (transverse waves). Sound waves can propagate only through matter, whereas electromagnetic waves propagate through a vacuum without attenuation. The speed of light is approximately 1 million times faster than the speed of sound in sea-level air. These high-frequency waves are capable of knocking electrons out of their orbits and can thereby cause cell injury and death or ontogenesis. The unknown concentration C is thus inversely proportional to the light path length d and directly proportional to the log of the ratio of incident to transmitted light intensity. Fortunately, both red and infrared light can penetrate soft tissues and may therefore be used to measure the concentrations of Hb species in vivo (see the section on "Processed Absorbance Monitors"). Small molecules absorb infrared light only if they have bonds and are asymmetric; in other words, their molecules have a dipole moment. Another limitation of infrared light is that ordinary glass absorbs it; therefore the measurement chambers for these devices must be made of sapphire or other infraredpermeable materials. In addition, when multiple substances are present, measuring their concentrations is still possible, provided enough wavelengths are available. Measuring the amount of light entering and exiting the system can determine the concentration of substances absorbing and reflecting light. The light absorbances of a mixture of gases can interfere with each other; consequently, compensations are built into current devices.