General Information about Cefuroxime
Cefuroxime, commonly recognized by its model name Ceftin, is an antibiotic medicine used for treating various bacterial infections. This powerful medication belongs to a bunch of antibiotics generally identified as cephalosporins and is particularly categorized as a second-generation cephalosporin. It is primarily used for treating infections in the respiratory system, urinary tract, pores and skin, and ears, making it a versatile and essential drug within the medical field.
In conclusion, Ceftin is a highly efficient medication that has confirmed to be a go-to for various bacterial infections. It supplies quick and environment friendly aid from symptoms, promoting a speedy recovery. However, it's crucial to use this medicine responsibly and with warning to keep away from any potential unwanted effects or drug resistance. Always consult a well being care provider before starting any medicine, and observe their instructions for the absolute best end result.
In addition to sinus infections, Ceftin can also be effective in treating skin infections like cellulitis and impetigo. These skin infections are brought on by micro organism penetrating the pores and skin's outer layer, leading to inflammation, redness, and ache. Ceftin successfully tackles these infections and prevents them from spreading, thus promoting quick and environment friendly therapeutic.
One of the most common makes use of of Ceftin is for sinus infections, that are brought on by bacteria coming into the sinus cavities and causing irritation. The signs of a sinus infection can be fairly uncomfortable, together with a blocked nose, headaches, and facial ache. Ceftin successfully targets the micro organism and relieves the symptoms, offering aid to the patient.
Ceftin belongs to the family of antibiotics which are similar to penicillin and works by interfering with the formation of the bacterial cell wall, thereby preventing the micro organism from rising and multiplying. This, in turn, leads to the eventual demise of the micro organism, thus curing the infection. The treatment is on the market in oral kind, as tablets and suspensions, making it convenient to use and simply accessible to sufferers.
Apart from these frequent infections, Ceftin can also be used to treat urinary tract infections (UTIs), which can happen in the bladder, kidneys, or urethra. UTIs are typically caused by bacteria entering the urinary tract, and Ceftin effectively targets these bacteria, relieving the discomfort and burning sensation experienced by sufferers. Additionally, Ceftin can be used to deal with Lyme illness, a bacterial an infection transmitted by way of tick bites, and gonorrhea, a sexually transmitted infection.
As with any medication, there are some precautions that have to be taken whereas using Ceftin. It is essential to disclose any known allergy symptoms or other underlying medical circumstances to the prescribing doctor to avoid any adverse reactions. Pregnant or lactating women also wants to seek the guidance of their doctor before taking Ceftin. Additionally, it is crucial to complete the total course of antibiotics prescribed, even if you begin feeling higher after a couple of days. Stopping the medication prematurely might result in the formation of antibiotic-resistant bacteria, making it more difficult to treat the infection in the future.
Furthermore, Ceftin can be helpful in treating infections in the respiratory system, similar to pneumonia, bronchitis, and tonsillitis. These infections could be attributable to a wide range of bacteria, and Ceftin targets them all, providing aid from signs like coughing, issue respiration, and sore throat. Ceftin is also effective in treating ear infections, which may be fairly common, especially among youngsters. By concentrating on the micro organism causing the an infection, Ceftin reduces the irritation and discomfort, permitting for a speedy recovery.
Although these associations are strong treatment effect definition 250 mg cefuroxime order with amex, the absolute risk of a malig nant complication is low, especially in patients who respond to a gluten-free diet. The diagnosis of celiac disease requires positive serologic markers and a compatible small-bowel biopsy. Celiac Disease Malabsorption can be a generalized process or can involve each specific nutrient class (carbohydrate, lipid, protein) indi vidually. For a discussion of the diagnosis and approach to fat malabsorption, see Diarrhea. Malabsorption Acute (<4 weeks) Chronic (>4 weeks) l l Secretory Inflammatory Malabsorptive Observation Stool cultures C. Celiac serologic studies may be negative in patients with lgA deficiency, in those with mild disease and limited small-bowel damage, and in those who have restricted dietary gluten. Other serologic studies, such as gliadin antibodies, have poor sensitivity and specificity and should not be used. However, these changes are not specific for celiac disease (Table 17); therefore, the diagnosis also relies on positive serologic tests. Symptom improvement often occurs within a few weeks, but histologic remission may take several months or years. Risk factors for a malignant complication include advanced age and long standing, poorly controlled disease. Repeat small-bowel biopsies are no longer required to show healing if there is a clear response to a gluten free diet; however, patients with atypical features at dis ease onset may benefit from follow-up histology to ensure mucosa! Mucosa] healing may take years in adults despite strict adherence to a gluten-free diet and may never be complete. Rightpanel: Histologic findings of celiac disease, with villous atrophy, crypt hyperplasia, and increased inflammatory infiltration of the lamina propria. Furthermore, this practice is expensive because endoscopy is required to obtain the sample. Conditions Associated with Small Intestinal Bacterial Overgrowth Disorders of Acid Secretion Achlorhydria Antrectomy/vagotomy Prolonged used of high-dose acid suppressive medications · the treatment of celiac disease is with a strict gluten free diet. In these cases, many clinicians use rotat ing antimicrobial agents (cycling between three to four differ ent classes) to avoid the development of bacterial resistance. Therefore, a lactose-free diet should be con sidered if the response to antimicrobial agents is incomplete. The colon can adapt to increase fluid and electrolyte absorption, and colonic bacteria can salvage malabsorbed nutrients through fermentation to short-chain fatty acids. Treatment focuses on ensuring adequate caloric, electrolyte, and fluid balance through the oral, enteral, and/or parenteral routes. Malabsorbed carbohydrates are fermented by colonic bacteria and produce osmotically active substances that cause diarrhea and gas, which causes bloating, discom fort, and flatulence. A careful dietary history is essential in the evaluation of a patient with chronic diarrhea. Lactose must be cleaved to glucose and galactose by the enzyme Jactase in the brush border of the small intestine in order to be absorbed. In many adults, the amount of Jactase present may be marginal or its expression is Jost, leading to lactose intolerance. The prevalence of lactose intolerance shows geographic and racial Carbohydrate Malabsorption · Short-bowel syndrome arises when a large portion of the small intestine is resected or diseased; it typically does not occur until less than 200 cm of healthy small intestine remains. For example, it is lowest in northern Europeans (approx imately 10%), more common in southern European and Middle Eastern populations (approximately 40%), and most common in Asian populations (up to 90%). Lactose intolerance is not absolute; patients are usually able to tolerate variable amounts of lactose. Lactose malabsorption often is diagnosed by history (bloating, cramps, and/or diarrhea related to dairy intake) and confirmed by resolution of symptoms with lactose avoidance. Treatment includes avoidance of lactose containing products or administration of lactase whenever dairy products are consumed. It is often overlooked because clinicians and patients do not recog nize the presence of fructose in many processed foods, typi cally in the form of high-fructose com syrup. Fresh fruits and fruit juices can also cause diarrhea if ingested in excess because the absorption of fructose has a maximum threshold. Fructose intolerance also may be diagnosed by careful history, including resolution of symptoms with dietary avoidance. Sugar alcohols (sorbitol, xylitol, maltitol, and others) are used as artificial sweeteners in sugar-free diet foods, candies, gums, and drinks. These carbohydrates have little or no absorption in the small intestine and, when taken in excess, cause symptoms of carbohydrate malabsorption. Breath tests exist for some sugar alcohols, but the diagnosis is generally made by a careful history. A variety of dietary factors have been proposed, but the results of studies in this area have been inconsistent. These factors are nonspecific and variable between patients, which may lead to diagnostic difficulty. A subset of patients has indeterminate colitis, which is characterized by clinical features and test results that do not allow a definitive classification. Inflammatory Bowel Disease · Fructose malabsorption is often overlooked because cli nicians and patients do not recognize the presence of fructose in many processed foods, typically in the form of high-fructose corn syrup. Some patients with distal inflammation can present with constipation owing to rectal spasm and stasis of stool. Severe disease may be characterized by fever, tachycardia, dehydration, abdominal tenderness, or pallor. Abdominal dis tention, hypoactive bowel sounds, and rebound tenderness suggest perforation or megacolon. Laboratory findings, such as significant anemia, leukocytosis, hypoalbuminemia, and elec trolyte abnormalities, also reflect the severity of disease.
A meta analysis of 1225 patients receiving 25% albumin after large volume paracentesis reported decreased postparacentesis circulatory dysfunction medications errors buy cefuroxime 500 mg fast delivery. Nonselective -blockers should be used with caution in patients with refractory ascites because there is an asso ciation with decreased survival. Midodrine can be used as adjunctive therapy for refractory ascites, especially in patients with hypotension. A polymorphonuclear cell count less than 250/µL with positive ascitic fluid cultures is diagnostic in symptomatic patients. Disorders of the Liver Cl Approximately 20% of hospitalized patients with cirrhosis develop acute kidney injury. Although most of these patients will respond to volume expansion, approximately 30% of this group will have hepatorenal syndrome. Therefore, hepatorenal syndrome accounts for a minority of patients who develop acute kidney injury. Patients who do not respond to these strategies and who meet criteria for hepa torenal syndrome should be treated for hepatorenal syndrome. Patients with type l hepatorenal syndrome should be treated with a vasoconslrictor and albumin. Terlipressin has been shown to improve kidney outcomes but is not availa ble in the United States. Patients with type I hepatorenal syndrome who clo not respond to medical therapy and are suitable candidates should undergo liver transplantation with or without simultaneous kidney trans plantation. Patients with type 1 hepatorenal syndrome who do not receive therapy usually die within Neeks. Cirrhosis of any cause is a risk factor for osteoporosis, with a prevalence of approximately 25%. Standard evaluation should include measurement of serum calcium, phosphate, and vitamin D levels. Patients with a previous fragility fracture, postmenopausal women, and those with glucocorti coid use for longer than 3 months should also receive dual energy x-ray absorptiometry. Osteoporosis should be managed with a bisphosphonate (after vitamin D repletion), which should be an intravenous formulation in patients with esophageal varices. Inactivated vaccines are safe in patients with cirrhosis, whereas attenuated live virus vaccines should be avoided. Table 34 describes the recommended vaccinations in patients with chronic liver disease and/or cirrhosis. Limited data exist regarding the efficacy and safety of vaccines against tetanus and diphtheria; Haemophilus inj1uenzae type b; measles, mumps and rubella; herpes zoster; and human papillomavi rus in patients with cirrhosis. Avoidances Hepatic osteodystrophy encompasses osteoporosis, osteope nia, and rarely osteomalacia in the context of liver disease. Concomitant inflamma tory bowel disease increases the risk of osteoporosis in Hepatic Osteodystrophy Health Care Maintenance of the Patient with Chronic Liver Disease Oysters and other raw shellfish should be avoided in patients with cirrhosis because there is a risk of potentially lethal infec tion with Vibrio vulnificus. Ds should be avoided owing to the risk of precipitating acute kidney injury and gastrointestinal bleeding. Occasional doses of acetaminophen are well tolerated in patients with cirrhosis but should never be used with alcohol. Complete cessation of alcohol use is recommended in all forms of chronic liver disease. Medications with significant risk of hepatoxicity, such as antituberculosis drugs 69 · Inactivated vaccines are safe in patients with cirrhosis, whereas attenuated live virus vaccines should be avoided. Fluid restriction is necessary in those with hypervolemic hyponatremia (serum sodium level of 125 mEq/L [125 mmol/L] or greater). Coffee may be benefi cial for liver health, but data are insufficient to make any spe cific recommendations. Most benign liver masses are discovered incidentally on abdominal imaging and only rarely result in symptoms. Lesions that are most likely to result in symptoms include abscesses or lesions larger than 5 cm, especially if subcapsular. The diagnosis of liver lesions can usually be made using imag ing, but biopsy is generally safe, even for vascular lesions. Ultrasound shows an anechoic structure with smooth, thin walls and posterior shadowing. Patients with autosomal dominant polycys tic kidney disease may also have multiple liver cysts that can cause symptomatic hepatomegaly. Hepatic Cysts · Most benign liver masses are discovered incidentally on abdominal imaging and only rarely result in symptoms. Adenomas may be subclassified depending on P-catenin (a proto-oncogene) nuclear reactivity on histologic specimens. Although malignant transformation of adenomas is unusual, those lesions that exhibit p-catenin nuclear reactivity are more likely to become malignant than those that are P-catenin negative. Adenomas larger than s cm have a risk of bleeding that can occasionally cause hemody namic compromise. Treatment with sur gical resection or radiofrequency ablation is advised for lesions that are larger than S cm (or larger than 3 cm when pregnancy is anticipated) or that exhibit P-catenin nuclear reactivity. Cl Pyogenic liver abscesses are usually due to peritonitis and biliary Hepatic Abscesses Amebiasis Hepatic amebic cysts are due to portal vein spread of intestinal infection to the liver. Patients with amebic cysts have either lived in or traveled to endemic areas such as India, Africa, or Central or South America. The diagnosis is usually established with compatible imaging and serologic testing. Treatment of the systemic infection with metronida zole or another appropriate agent should be following by a luminal agent such as paromomycin. Most patients present with fever and symptoms owing to the underlying cause of the abscess.
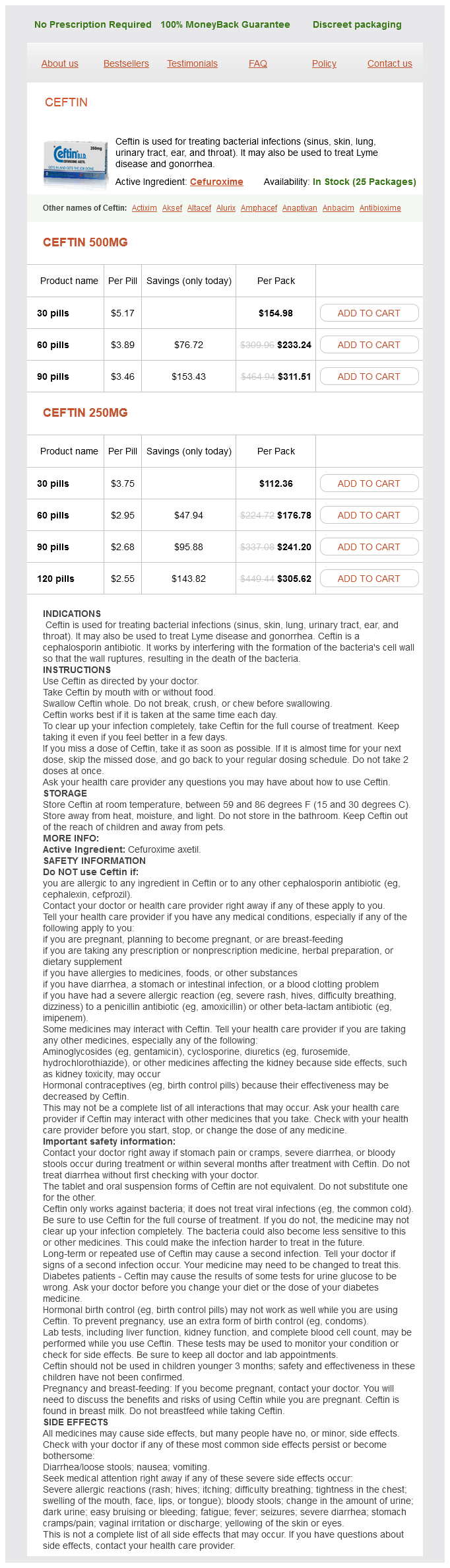
Cefuroxime Dosage and Price
Ceftin 500mg
- 30 pills - $154.98
- 60 pills - $233.24
- 90 pills - $311.51
Ceftin 250mg
- 30 pills - $112.36
- 60 pills - $176.78
- 90 pills - $241.20
- 120 pills - $305.62
Item 23 In addition to starting nigh-flow supplemental oxygen treatment nail fungus cefuroxime 250 mg with visa, wnich of the following is the most appropriate manage ment She has had asthma since childhood, but her asthma symptoms have progressively worsened recently. Over the past 2 years, she has had twice-yearly visits to the emergency department requiring treatment with pro longed glucocorticoid tapers. She has no symptoms of gastroesophageal reflux, sinus disease, or other symp toms, and she diligently avoids environmental exposures and likely triggers. Medical history is significant for multiple allergies; skin testing has been positive for allergy to dust mites, cats, and ragweed. Medica tions are a high-dose inhaled glucocorticoid, a long-acting p1-agonist, a leukotriene antagonist, a long-acting anticho linergic agent, and an as-needed short-acting P1-agonist. Her medical history is notable for long-standing type 2 diabetes mellitus controlled by diet. Laboratory studies reveal normal hemoglobin, serum electrolyte, and serum creatinine levels. Ventilator settings are unchanged rrom the operating room: volume controlled continuous mandatory ventila tion (assist control) mode with a respiration rate ort6/min. Blood pres sure is 140 88 mm Hg, pulse rate is 90/min, and respiration rate is J61 11in. Cardiac ex8minalion reveals a grade 2 6 early systolic murmur over the aortic area. Other than postoperative changes, the remainder or the physicaI exa111ination is normal. Her oxygen requirement also inci·eascs despite diuresis with a negative fluid balance. He initially presented with increas ing dyspnea and a constant dull ache on his right side. Initial chest radiograph showed a moderate-sized, free-flowing pleural effusion on the right; the left lung field was unremarkable. A repeat tho racentesis performed 2 weeks later showed similar results, also with negative cultures and cytology. Dullness to percussion and decreased breath sounds are noted over the lower third of the right hemitho rax. He is being evaluated after several days off from work and currently has no symptoms or medical concerns. The sinus examination is normal and the lungs are clear, with no wheezing or crack les noted. Item 29 Which of the following is the most appropriate diagnostic test to perform next Oropharyngeal examination reveals patent nasal airways, a low-lying soft palate, and a slight dental overjet. Item 30 Self-Assessment Test Which of the following is the most appropriate alternative treatment to continuous positive airway pressure Symptoms began fol lowing initiation of her latest round of chemotherapy for treatment of non-Hodgkin lymphoma l week ago. Subcutaneous low-molecular weight heparin is begun for venous thromboembolism prophylaxis. On the morning of the third hospital day, she is found unresponsive in her hospital room. His symptoms began 6 months ago when he noted the paroxysmal onset of persistent coughing spells that make it difficult to carry on a conversation. He was initially diagnosed with allergic rhinitis and was started on a glucocorticoid nasal inhaler with some improvement of his rhinitis symptoms but not his cough. Medications are a fluticasone nasal inhaler and an over-the-counter antihistamine as needed. Slight nasal congestion and dry cough are noted during examination, but both are improved from his previous evaluation. He has had two exacerbations in the past year requiring hospitalization, and his baseline exercise tolerance is low. He completed pulmo nary rehabilitation 3 months ago without much improve ment in exercise capacity. His medications are tiotropium, fluticasone/salmeterol, daily roflumilast, and albuterol as needed. His 6-minute walking distance is 240 meters (787 feet), consis tent with decreased exercise tolerance. His medications are a tiotropium inhaler, an albuterol/ipratropium inhaler, aspirin, rosuvastatin, and metoprolol. Pulmonary examination reveals distant breath sounds, resonance to percussion, and no wheeze. He has a history of chronic atrial fibrillation and heart failure with stable exertional dyspnea. A 30-year-old woman is evaluated in follow-up for wheez ing and cough that started 6 weeks ago after a viral respira tory illness. At that time she had daily wheezing and cough with nocturnal symptoms that would disturb her sleep. Her daytime symptoms of wheezing and cough have resolved, but she notes that she awakens from sleep with shortness of breath approximately twice a week. Medical history is notable for mild asthma as a child that was treated for several years; however, she has not required treatment since age 15 years. Item 36 (A) Arterial blood gas studies (B) Echocardiographic assessment of pulmonary artery pressures (C) Hypoxia altitude simulation test (D) Recommend not flying A 74-year-old man is evaluated in follow-up for a diagno sis of silicosis related to his former occupation as a mine worker.