General Information about Bentyl
Bentyl, additionally identified by its generic name Dicyclomine, is a medication used to deal with the signs of IBS. It belongs to a gaggle of medication known as antispasmodics, which work by relaxing the muscles in the digestive tract, thereby lowering cramping, pain, and discomfort. It is on the market within the type of tablets, capsules, and injectables, and it can be taken with or without meals.
Before taking Bentyl, it is essential to consult a well being care provider for a proper analysis and to determine if it's the right treatment for you. It isn't really helpful for people with sure situations like glaucoma, myasthenia gravis, or an enlarged prostate. It can additionally be not suitable for many who have a historical past of diarrhea attributable to an an infection. Pregnant and breastfeeding ladies should also seek the guidance of their doctors earlier than taking Bentyl.
Bentyl is mostly well-tolerated, but like any other medicine, it might cause unwanted effects in some individuals. The most commonly reported side effects include dry mouth, dizziness, drowsiness, blurred vision, and issue urinating. These unwanted facet effects are often mild and subside with continued use. However, in the occasion that they persist or turn out to be severe, it is very important inform your physician.
Irritable bowel syndrome (IBS) is a standard digestive dysfunction that impacts hundreds of thousands of people worldwide. It is characterized by symptoms corresponding to stomach ache, bloating, constipation, and diarrhea. IBS can have a major impact on an individual's quality of life, making it difficult to hold out day by day activities and disrupting day by day routines. The excellent news is that there are remedies obtainable to alleviate these symptoms, and one of them is Bentyl (Dicyclomine).
Bentyl has been proven to be effective in treating the symptoms of IBS, but it is not a remedy for the condition. It should be used as part of a comprehensive treatment plan that features way of life changes such as a nutritious diet, regular exercise, and stress management strategies. These adjustments, mixed with Bentyl, can significantly enhance the signs of IBS and assist patients lead a more comfortable and fulfilling life.
In conclusion, Bentyl (Dicyclomine) is a trusted and effective medicine for managing the signs of IBS. It works by targeting the underlying causes of the situation, offering much-needed relief from the discomfort and ache associated with it. If you suffer from IBS, seek the guidance of your physician about Bentyl and its suitability for you. With correct use and at the facet of life-style adjustments, Bentyl can help you manage your symptoms and enhance your overall high quality of life.
The dosage of Bentyl may vary from individual to individual, based mostly on the severity of their signs. It is normally taken 4 instances a day, however your doctor might advocate a unique schedule relying in your situation. It is important to comply with the prescribed dosage and to not exceed it, as taking an extreme quantity of can lead to adverse effects. If you miss a dose, take it as soon as you keep in mind, but whether it is virtually time for the next dose, skip the missed dose and resume your regular dosing schedule.
In rare instances, Bentyl can cause more critical unwanted effects, corresponding to an allergic reaction, tachycardia (rapid heart rate), issue respiratory, or swelling of the face, lips, tongue, or throat. If you expertise any of those signs, search instant medical consideration.
The precise reason for IBS remains to be unknown, however it's believed to be a combination of factors such as abnormal muscle contractions within the intestine, nerve dysfunction, and inflammation of the intestine. Bentyl helps to address these underlying points by concentrating on the muscle tissue and nerves in the digestive tract, providing aid from the signs of IBS.
If clinical signs or symptoms persist or recur gastritis fish oil purchase cheap bentyl online, or titer does not fourfold, patient should be treated again for presumed treatment failure or reinfection. Rocky Mountain Spotted Fever Rickettsia rickettsii transmitted by bite of Dermacentor tick. Type of dog tick, much larger, and more likely for patient to discover, than the tick that transmits Lyme disease. Despite name of disease, Dermacentor ticks and Rickettsia rickettsii are broadly distributed, with most common areas being mid-Atlantic and South Central states. Neurologist may become involved because of severe headaches, significant mental status changes, coma and ultimately death if the diagnosis not made. Confirmation of diagnosis can be obtained by serological testing and/or biopsy of skin lesions. Prognosis: Usually fatal within 85 days of symptom onset if left untreated; full recovery if properly treated. Prion-Related Diseases A 40-year-old man developed progressive worsening of anxiety and depressed mood with auditory and visual hallucinations. His clinical status progressively deteriorated over the next 13 months with decreased cognitive function with some chorea followed by myoclonus. The onset usually occurs between the ages of 45 and 75, with the peak onset between 60 and 65. Prodromal symptoms include fatigue, insomnia, depression, weight loss, and headaches, but mental deterioration and myoclonus frequently present with some extrapyramidal signs, cerebellar ataxia, and cortical blindness. Also transmitted among Fore tribes of New Guinea via ritualistic cannibalism, in which case disease is termed kuru. There are other rare genetic forms, such as Gerstmann-Straussler disease and fatal familial insomnia. Other symptoms include personality changes, anxiety, depression, paranoia, obsessive-compulsive symptoms, hallucinations, and psychosis. Patients will also often develop motor manifestions, including both pyramidal and extrapyramidal signs and symptoms. Startle myoclonus is common, but often does not appear until late in disease course. Special cautions must be taken to prevent transmission when brain biopsy is done on any patient with suspected prion disease. Psychiatric manifestations typically precede neurologic manifestations, and patients are usually initially thought to have primary psychiatric disorder. Neurologic symptoms develop about 6 months after psychiatric onset, and include dementia, akinetic mutism, painful sensory symptoms, ataxia, involuntary movements. Endemic to Central and South America and being seen with frequency in the United States among immigrants from that part of the world. Treatment: Albendazole or praziquantel, sometimes with steroids; anticonvulsants as needed. Different sensory receptors have different functions: Pacinian corpuscles: Deep pressure, touch, high-frequency vibration. Myofibers are extrafusal or intrafusal: Extrafusal fibers: Contraction across joints. Type I: Slow-twitch, fatigue resistant, naturally darker, low in glycogen, high in oxidative enzymes. Disorders of Roots, Plexus, and Nerve A 73-year-old man presents with several years of gradual, symmetric numbness and tingling that started in his toes. What feature of the exam would most convincingly show that his problem is peripheral, not central Consider when sensory disturbance is non-length-dependent, with prominent ataxia and no weakness. Genitourinary (recurrent urinary tract infection, erectile dysfunction, incontinence/nocturia/urgency/hesitancy). Cervical Radiculopathies symptoms (see table 11-4) Pain in neck, shoulder, arm-often vague localization. Spurling sign: Neck extension and rotation toward symptomatic side reproduces radicular symptoms. The arcade of Frohse is pictured on the radial nerve; the carpal tunnel is pictured on the median nerve; and Guyon canal is pictured on the ulnar nerve. Most common cause is compression by disk protrusion, ligament hypertrophy, spondylolisthesis. C6 Shoulder abduction, shoulder external rotation, elbow fl xion, forearm pronation, wrist extension, radial wrist fl xion. Upper Brachial Plexopathies symptoms/exam Weakness: C5-innervated muscles (deltoid, supra/infraspinatus, biceps, brachialis; very proximal injury; serratus anterior and/or rhomboids). Birth injury ("Erb-Duchenne palsy") due to traction of the head and neck away from the shoulder. Any injuries involving downward displacement of the shoulder/arm and/or lateral displacement of the head and neck. Causes treatment Lower Brachial Plexopathies symptoms/exam Weakness of C81-innervated muscles (the intrinsic hand muscles). Clue to lower trunk lesion: Atrophy of thenar eminence with sensory loss in medial hand/fingers.
At present gastritis diet ������� purchase bentyl from india, humidity measurements have not been introduced in clinical practice as the implications of such measurements are not clear. One reason for this is to avoid a medicolegal conflict if a patient claims a decreased sense of smell postoperatively. Warming-Up Capacity the same applies to measuring the warming-up capacity of the nose. Tests to determine the humidifying and the warming-up capacity of the nose will be introduced in the future. The test substance must not interact with mucus or the mucosal membrane, and it must be easily detectable in the nasopharynx. The arrival of a dye in the nasopharynx is established by posterior rhinoscopy using a rigid endoscope. When saccharine is used, the test subject is asked to inform the examiner as soon as he or she notices a sweet taste. The transport of technetium is determined by measuring radioactivity with a gamma camera. The combination of charcoal and saccharine is most commonly used in a clinical setting. Radioactive technetium is advocated for research purposes, as it is the most sensitive method. Ciliary Beat Observation and Measurement of Ciliary Beat Frequency Ciliary function can be examined by phase-contrast microscopy or by studying ciliary beat using a photoelectric method. A brush or a small biopsy is taken from the medial surface of the inferior turbinate without the use of any local anesthetic or decongestants, as these drugs are known to affect ciliary activity. The brush or biopsy is best stored and examined in Locke-Ringer solution (sodium chloride, potassium chloride, calcium chloride, magnesium chloride, sodium bicarbonate, and dextrose in water), not in isotonic (0. Charcoalaccharine Test A small amount of charcoal and saccharine is deposited just posterior to the head of the inferior turbinate. The method records the time elapsing until the charcoal becomes visible in the choana (as observed by posterior rhinoscopy with a rigid 70endoscope) and/or until the saccharine is tasted. Technetium Test this technique is a more precise method and is therefore preferred for clinical research. It is more cumbersome and requires the assistance of a department of nuclear medicine. When structural anomalies like missing dynein arms are observed, the diagnosis of ciliary akinesia is very likely. The patient is asked about any of the following reactions: Nasal symptoms like nasal congestion, rhinorrhea, secretions, and itchy nose Ocular symptoms like itchy eyes, tearing and/or conjunctival vascular dilation Bronchial symptoms like cough, shortness of breath, and wheezing Cutaneous problems like atopic eczema, itchy and red skin General problems like impaired sleep, disturbed concentration and/or reduced physical activity the patient is also interviewed about abnormal nasal responses to specific stimuli such as temperature changes, air pollution (smoke, dust), food, drink, and light. Allergy testing is an integral part of the routine diagnosis of patients with nasal mucosal disease. A small amount of an inert compound is deposited just posterior to the head of the inferior turbinate (or on the septum at the level of the valve area). The time that elapses until the test substance arrives in the nasopharynx is measured. Hyperreactivity may be tested by provocation of the nasal mucosa with histamine (histamine diphosphate 330/nostril), methacholine, or cold dry air. These tests have not yet come into clinical practice due to their timeconsuming nature. Each method has its intrinsic advantages and disadvantages that should be taken into account. Rhinology 1984;22:1515 and Consensus report on acoustic rhinometry and rhinomanometry. The nose evolved to facilitate smelling and breathing, to detect odors, to control the inspiratory and expiratory airstream, to humidify and warm inspired air, and to serve as the first line of defense of the respiratory tract. These functions are taken care of by the interaction between the inspired air and the mucous membranes. This interaction is made possible by the complex airflow through the nose, determined by the geometry of the internal nose and by its external form. Nowadays, a large proportion of all nasal surgery is done in pursuit of the elusive goals of beauty and happiness. It is telling that most books on nasal surgery that have appeared over the past decades are devoted to cosmetic rhinoplasty. No matter how legitimate the pursuit of beauty may be, the nasal surgeon should be aware of the limits of surgery. A special effort is made to preserve mucosal membrane, the functional organ of the nose. If the turbinates are to be reduced, the required reduction in volume is achieved by a method that ensures preservation of their function. Apart from exceptional cases, septal and pyramid pathology are addressed in one procedure. The bony pyramid can therefore only be successfully repositioned after mobilization and repositioning of the septum. Similarly, deformities of the cartilaginous pyramid can only be adjusted after mobilization of the septum. First, the septum has to be rebuilt to provide support for the dorsum, tip, and columella. Finally, the lobule is modified as required, and adjusted to the new septum and pyramid.
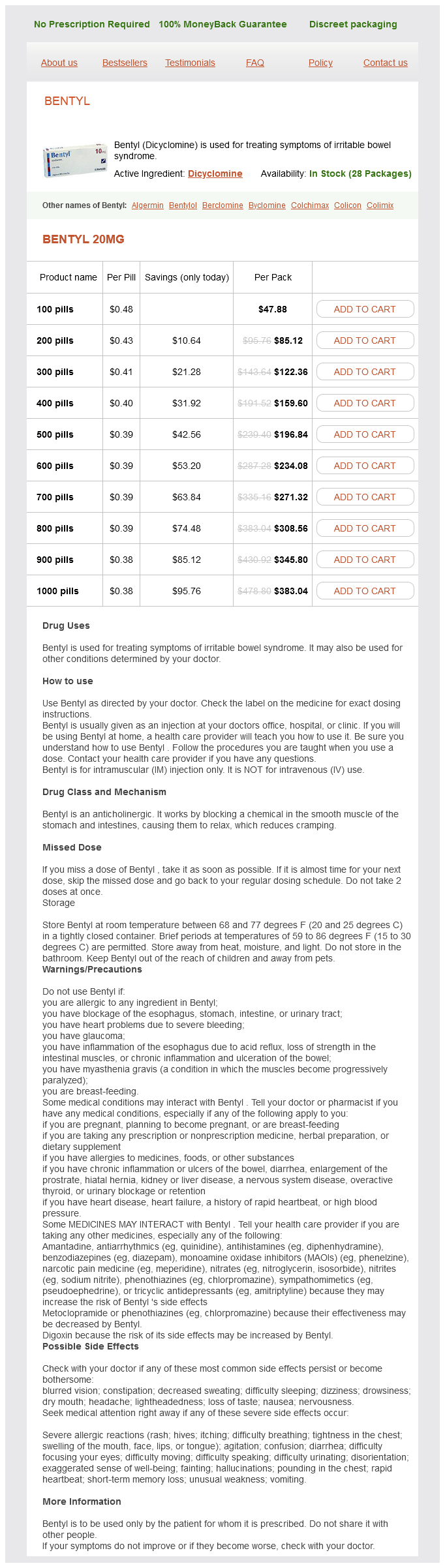
Bentyl Dosage and Price
Bentyl 20mg
- 100 pills - $47.88
- 200 pills - $85.12
- 300 pills - $122.36
- 400 pills - $159.60
- 500 pills - $196.84
- 600 pills - $234.08
- 700 pills - $271.32
- 800 pills - $308.56
- 900 pills - $345.80
- 1000 pills - $383.04
Prosopagnosia: Bilateral (or large unilateral) lesion of the ventral occipitotemporal lobes chronic gastritis what to eat best buy bentyl. Akinetopsia: Inability to perceive moving objects, but objects can be recognized once they are stationary. Fibers from cochlear nuclei: Dorsal cross the pontine tegmentum contralateral lateral lemniscus. Ventral synapse bilaterally in superior olivary nucleus complex bilateral lateral lemnisci. Medial geniculate nucleus: Receives fibers from the inferior colliculus in the brachium of the inferior colliculus. Because the auditory pathway above the cochlear nuclei represents parts of the sound input to both ears, a unilateral lesion in the lateral lemniscus, medial geniculate body, or auditory cortex does not result in marked loss of hearing on the ipsilateral side. The superior olivary nucleus is responsible for localizing sounds horizontally in space. Semicircular canal (superior, lateral, and posterior): Responds to angular acceleration and deceleration. Vestibulospinal Tracts Lateral: Goes to entire ipsilateral spinal cord (involved in postural control). Medial: Goes to contralateral cervica and thoracic cord (involved in head positioning). Pyriform cortex (thalamus) frontal lobe; this tract is responsible for conscious detection of odors. Medial olfactory stria anterior olfactory nucleus (which communicates back to the olfactory bulbs) and anterior perforated substance; olfactory reflex reactions. Taste fibers nucleus solitarius (in medulla) ventral posteromedial thalamus primary gustatory cortex in the opercular and insural regions of the frontal lobes, secondary gustatory cortex in caudolateral orbitofrontal cortex, amygdala, hypothalamus, and basal forebrain. Primarily located in medial and ventral portions of the frontal and temporal lobes. The cortical parts of the limbic system, or limbic lobe, are interconnected by a septo-hypothalamic-mesencephalic bundle, ending in the hippocampus, and the fornix, which runs from the hippocampus back to the mamillary bodies, and by tracts from the mamillary bodies to the thalamus and from the thalamus to the cingulate gyrus. Major Limbic Pathways PathWay Fornix inPut Subiculum Hippocampus Hippocampal formation Medial septal nucleus Nucleus of diagonal band outPut Medial and lateral mammillary nuclei; lateral septal nuclei Lateral septal nuclei Anterior thalamic nucleus Hippocampal formation Hippocampal formation Anterior thalamic nucleus Parahippocampal gyrus Brain stem Habenula Contralateral anterior olfactory nucleus Contralateral amygdala Contralateral anterior temporal cortex Hypothalamus Septal nucei Brain stem nuclei Amygdala, other forebrain structures Dentate gyrus granule cells Hippocampal pyramidal cells Mammillothalamic tract Cingulum Mammillotegmental tract Stria medullaris Anterior commissure Medial mammillary nucleus Cingulate gyrus Mammillary bodies Medial septal nuclei Anterior olfactory nucleus Amygdala Anterior temporal cortex Stria terminalis Corticomedial amygdala Amygdala Medial forebrain bundle Amygdala, other forebrain structures Brain stem nuclei Perforant pathway Alvear pathway Entorhinal cortex Entorhinal cortex Hippocampal formation: Primary functions in memory. Schematic illustration of the major connections to , within, and from the hippocampal formation. Subthalamus: Lies between dorsal thalamus and tegmentum, consists of the subthalamic nucleus. Thalamic White Matter Thalamic radiations: Fiber bundles that emerge from the lateral surface of the thalamus and terminate in cerebral cortex. Internal medullary lamina: Vertical sheet of white matter that bifurcates in its anterior portion and divides the gray matter of the thalamus into lateral, medial, and anterior nuclear groups. Input: Mammillary bodies of hypothalamus via mamillothalamic tract; hippocampus via fornix. Output: To hypothalamus; sends a massive projection to cingulate and orbitofrontal cortex. Output: To primary motor cortex (area 4) and premotor and supplementary motor cortex (area 6). Output: To primary motor cortex (area 4) and premotor/supplementary motor cortex (area 6). Output: To primary visual cortex (area 17) via the optic radiations (receives a good deal of feedback input from the cortex). Input: From parietal and temporal association areas, which include secondary association cortices devoted to vision, somatosensation, and audition, from superior colliculus and primary visual cortex. Output: To parietal and temporal association areas, which include secondary association cortices devoted to vision, somatosensation, and audition. Role: Integration of sensory information and in the modulation of spatial attention. Role: Regulate flow of information from the thalamus to the cortex, part of the ascending reticular activating system, modulation of arousal and sleep and in the generation of brainwave activity. Hypothalamic Nuclei nucLeus Lateral Hypothalamus Lateral hypothalamic nucleus function Induces eating when stimulated. Medial Hypothalamus Preoptic region Median preoptic nucleus Anterior nucleus Lateral preoptic nucleus Supraoptic region Supraoptic nucleus Paraventricular nucleus Suprachiasmatic nucleus Tuberal region Ventromedial nucleus Arcuate nucleus Mammillary region Mammillary nucleus Input from hippocampal formation via fornix. Dorsomedial nucleus Posterolateral nucleus Involved in behavior control, when stimulated leads to violent behavior in animals. Projects to cholinergic and monoaminergic neurons in brain stem and lateral preoptic nucleus. Posterior Hypothalamus Posterior hypothalamic nucleus Involved in thermoregulation. Anterior limb: Separates the putamen and globus pallidus from the caudate nucleus. Contains the following fiber bundles: thalamocortical and corticothalamic fibers that course between lateral thalamic nuclear group and frontal lobe cortex. Contains the following fiber tracts: corticobulbar and corticospinal tracts run in anterior one-half of the posterior limb, with fibers to the face at genu of the internal capsule. Corticorubral fibers from the frontal lobe cortex to the red nucleus accompany the corticospinal tract. Somatosensory fibers from thalamus to the postcentral gyrus of cortex lie in the posterior one-third of the posterior limb.