General Information about Antabuse
Antabuse, also referred to as disulfiram, is a medicine used for the therapy of alcoholism. This drug works by inflicting disagreeable results when alcohol is consumed, which acts as a deterrent for people struggling with alcohol dependancy. Antabuse doesn't treatment alcoholism, however it can be a helpful tool within the recovery process.
Antabuse has been used as a remedy for alcoholism because the Nineteen Forties. It was initially used to deal with parasitic infections, but its effects on alcoholism have been found by chance. Researchers seen that patients experienced opposed reactions once they consumed alcohol whereas taking the treatment. This led to the event of Antabuse as a remedy for alcohol addiction.
If a person taking Antabuse consumes alcohol, they will expertise a spread of signs that may final for several hours. These signs can be harmful and, in some circumstances, life-threatening, such as heart palpitations, low blood pressure, and difficulty breathing. Therefore, it's essential to follow the doctor's instructions and avoid any alcohol-containing merchandise while taking Antabuse.
The concern of experiencing these disagreeable results could be a highly effective deterrent for individuals struggling with alcohol habit. Knowing that they may really feel ill in the event that they devour alcohol can help them resist the urge to drink. However, it's important to note that Antabuse doesn't treat the habit itself. It merely helps individuals keep sober by making alcohol consumption less fascinating.
Alcoholism is a serious and continual disease that affects hundreds of thousands of people worldwide. It is characterized by a robust yearning for alcohol, an inability to control alcohol consumption, and a bodily dependence on the substance. Alcoholism can have extreme consequences on an individual's well being, relationships, and total high quality of life. Therefore, looking for therapy for alcohol dependancy is essential for these affected.
In conclusion, Antabuse is an efficient medication for individuals fighting alcoholism. It works by causing disagreeable effects when alcohol is consumed, which serves as a deterrent for these in restoration. However, it is crucial to do not neglect that this medication is solely one a half of a comprehensive treatment program for alcohol habit. It requires dedication and a strong commitment to sobriety for individuals to attain long-term recovery. If you or someone you understand is struggling with alcoholism, seek help from a medical professional to discuss if Antabuse could additionally be a useful treatment choice.
Antabuse is prescribed for use as part of a complete treatment program for alcoholism. It is usually combined with counseling, support groups, and different therapies to handle the underlying causes of dependancy. This medicine is typically used in the first few months of treatment when an individual's motivation to stay sober could also be at its weakest. It helps construct a basis for sobriety and teaches individuals how to cope with their dependancy triggers.
It is essential for patients to grasp that Antabuse isn't a magic pill that will remedy their alcohol habit. It requires a strong commitment to sobriety and way of life adjustments to realize long-term restoration. Some individuals may experience side effects from Antabuse, corresponding to drowsiness, headaches, or pores and skin rash. It is crucial to inform one's doctor if these unwanted facet effects turn into bothersome or extreme.
The method Antabuse works is by inhibiting an enzyme referred to as aldehyde dehydrogenase, which is answerable for breaking down alcohol in the physique. As a result, when an individual takes Antabuse and consumes alcohol, their body is unable to metabolize it properly. This results in a build-up of a toxic substance known as acetaldehyde, which causes a spread of disagreeable symptoms corresponding to flushing, sweating, nausea, vomiting, and headache.
In the elderly symptoms nausea headache buy generic antabuse online, fewer functional symptoms such as anxiety, stress, and unrefreshed sleep are present. However, the elderly have more musculoskeletal complaints than their younger counterparts. Providing patients with literature regarding their illness and explaining to them that they are indeed dealing with a real disorder is an ideal starting point. At the same time, patients need to be reassured that they are dealing with a nondestructive, although not necessarily benign, illness. Response to treatment can be assessed in a variety of ways as suggested in a review by Bennett. If depression is an issue, this can be monitored using a daily diary or the Beck Depression Inventory. All patients are expected to develop dependency; that is, these drugs cannot be abruptly withdrawn without causing unpleasant side effects such as pruritus, nausea, and drowsiness. Frequent re-evaluation of the patient is especially important in this setting, with the goal being improved function rather than mere pain relief. If improved function is not achieved, if severe side effects are encountered, or if maladaptive behavior develops, patients should be weaned from these agents and not restarted on them. Seizures have been reported, especially when this agent is combined with antidepressants. Ferraccioli and colleagues found improvements lasting up to 6 months in patients treated with electromyographic biofeedback. Buckelew and colleagues found that biofeedback in conjunction with low-impact exercise produced better results than each of the modalities on its own. Haanen and colleagues showed significant improvement in five outcome measures in a group treated with hypnotherapy as compared with a physical therapy program. A combination of fluoxetine and amitriptyline was found to be more effective than either agent alone or placebo. Miscellaneous Agents 2-Adrenergic agonists such as tizanidine have been used successfully in chronic pain disorders. These drugs have been used in the control of nausea and vomiting in patients who have received chemotherapy or radiation. Pregabalin, an anticonvulsant with analgesic properties, has been shown to produce global improvement in a large (459 patient) placebo-controlled trial at a dose of 450 mg a day. The nonselective serotonin reuptake inhibitors with a noradrenergic component, such as venlafaxine, nefazadone, and bupropion, are better tolerated in this group of patients. There is also no evidence of pathologic abnormalities at tender points or trigger points. Neurohormonal dysregulation might result in abnormal blood flow to some areas of the brain that regulate pain perception, such as the thalamus and caudate nucleus. Natural history reports indicate that complete remissions are unusual and that patients continue to be symptomatic, but gradual and modest improvement with time is common. Each of these entities might fit into a psychosocial rather than a biomedical model. TreatmentofSpecificSymptoms Sleep Before pharmacologic treatment is initiated, certain measures must be tried. Caffeinated beverages should be avoided 4 to 6 hours before the patient goes to bed. Relaxation techniques such as yoga, gentle stretching, or listening to soothing music are all helpful. Pure sedatives such as benzodiazepines, antihistamines, and antidepressants are the pharmacologic therapies available. Care should be taken when clonazepam is used on a long-term basis because it causes prominent withdrawal symptoms when discontinued abruptly. Specific symptoms should be sought in the history that point to a diagnosis of sleep apnea, because this diagnosis is often missed. The pathophysiology of fibromyalgia syndrome is intimately related to the effects of psychological distress and disordered sleep on the central nervous system. The simple, effective approach to treatment employs the combination of patient education, improved mood and sleep, and aerobic exercise. Goldenberg D, Mayskiy M, Mossey C, et al: A randomized, double-blind crossover trial of fluoxetine and amitriptyline in the treatment of fibromyalgia. Mease P: Fibromyalgia syndrome: Review of clinical presentation, pathogenesis, outcome measures, and treatment. The clinical course of gout can be summarized into the stages of acute intermittent gout and chronic tophaceous gout. Hyperuricemia is the underlying metabolic aberrancy in gout and is defined as the serum urate level, in body fluids, above which urate precipitates into monosodium urate crystals. Prevalence Gout is a fairly common disease, more common in men than women, and rare in premenopausal women. In a population of medical students with a median age of 22 years, the cumulative incidence of gout was reported as 8. Therefore, when the human body is unable to eliminate large burdens of urate, hyperuricemia develops. As urate levels increase and saturate the synovial fluid or soft tissues, crystals precipitate, leading to tissue damage and the development of tophi. After urate crystals deposit in soft tissues and joints, monocytes and macrophages are activated in an attempt to clear the crystals by phagocytosis. This then leads to the release of proinflammatory cytokines and chemokines into the surrounding area, triggering a cascade of acute inflammatory reaction and influx of neutrophils into the joint, for example.
It is seen in focal bacterial or medications you can give dogs purchase generic antabuse on line, occasionally, fungal infections, because microbes stimulate the accumulation of leukocytes and the liberation of enzymes from these cells. The necrotic material is frequently creamy yellow because of the presence of leukocytes and is called pus. For It is useful to consider the possible events that determine when reversible injury becomes irreversible and progresses to necrosis. The clinical relevance of this question is obvious- if we can answer it, we may be able to devise strategies for preventing cell injury from having permanent deleterious consequences. The areas of white chalky deposits represent foci of fat necrosis with calcium soap formation (saponification) at sites of lipid breakdown in the mesentery. Gangrenous necrosis is not a specific pattern of cell death, but the term is commonly used in clinical practice. It is usually applied to a limb, generally the lower leg, that has lost its blood supply and has undergone necrosis (typically coagulative necrosis) involving multiple tissue planes. When bacterial infection is superimposed, there is more liquefactive necrosis because of the actions of degradative enzymes in the bacteria and the attracted leukocytes (giving rise to so-called wet gangrene). Caseous necrosis is encountered most often in foci of tuberculous infection (Chapter 8). The term caseous (cheeselike) is derived from the friable white appearance of the area of necrosis. On microscopic examination, the necrotic area appears as a structureless collection of fragmented or lysed cells and amorphous granular debris enclosed within a distinctive inflammatory border; this appearance is characteristic of a focus of inflammation known as a granuloma (Chapter 3). Fat necrosis refers to focal areas of fat destruction, typically resulting from release of activated pancreatic lipases into the substance of the pancreas and the peritoneal cavity. This occurs in the calamitous abdominal emergency known as acute pancreatitis (Chapter 19). In this disorder, pancreatic enzymes leak out of damaged acinar cells and liquefy the membranes of fat cells in the peritoneum, releasing triglyceride esters that are split by pancreatic lipases. Fatty acids are generated that combine with calcium to produce grossly visible chalky-white areas (fat saponification), which enable the surgeon and the pathologist to identify the underlying disorder. On histologic examination, the necrotic areas contain the shadowy outlines of necrotic fat cells, basophilic calcium deposits, and an inflammatory reaction. Fibrinoid necrosis is a special form of vascular damage usually seen in immune reactions involving blood vessels. It typically occurs when complexes of antigens and antibodies are deposited in the walls of arteries. Deposits of these immune complexes, together with plasma proteins that has leaked out of vessels, result in a bright pink and amorphous appearance in H&E stains called "fibrinoid" (fibrin-like) by pathologists. The immunologically mediated vasculitis syndromes in which this type of vascular injury is seen are described in Chapter 11. Tuberculosis of the lung, with a large area of caseous necrosis containing yellow-white and "cheesy" appearing debris. The wall of the artery shows a circumferential bright pink area of necrosis with inflammation (neutrophils with dark nuclei). If necrotic cells and cellular debris are not promptly destroyed and reabsorbed, they provide a nidus for the deposition of calcium salts and other minerals and thus tend to become calcified. This phenomenon, called dystrophic calcification, is considered later in the chapter. Apoptosis in Physiologic Situations Death by apoptosis is a normal phenomenon that serves to eliminate cells that are no longer needed, or as a mechanism to maintain a constant number of various cell populations in tissues. Central to this process is death of cells by apoptosis and their removal by phagocytes. Apoptosis is important in the following physiologic situations: the removal of supernumerary cells (in excess of the required number) during development. Cell death is critical for involution of primordial structures and remodeling of maturing tissues. Apoptosis is a generic term for this pattern of cell death, regardless of the context, while programmed cell death refers only to apoptosis during development. In all of these situations, cells undergo apoptosis because they are deprived of necessary survival signals, such as growth factors and interactions with the extracellular matrix, or they receive pro-apoptotic signals from other cells or the surrounding environment. Apoptotic cells break up into plasma membranebound fragments, called apoptotic bodies, which contain portions of the cytoplasm and nucleus. While the plasma membrane remains intact, its surface components are altered so as to produce "find me" and "eat me" signals for phagocytes, discussed later. As a result, the dead cell and its fragments are rapidly devoured, before the contents leak out, and therefore apoptosis does not elicit an inflammatory reaction. Apoptosis was first recognized in 1972 by the distinctive morphologic appearance of membrane-bound fragments derived from cells, and named after the Greek designation for "falling off. This phenomenon, termed programmed cell death, is controlled by the action of a small number of genes and is required for normal embyrogenesis. Thus, apoptosis is a unique mechanism of cell death, distinct from necrosis in many respects. Apoptosis in Pathologic Conditions Apoptosis eliminates cells that are injured beyond repair without eliciting a host reaction, thus limiting collateral tissue damage. If repair mechanisms cannot correct the damage, the cell triggers intrinsic mechanisms that induce apoptosis. An important host response to viruses consists of cytotoxic T lymphocytes Causes of Apoptosis Apoptosis occurs in two broad contexts: as part of normal physiologic processes, and as a pathophysiologic mechanism of cell loss in many different diseases. This contrasts with necrosis, in which an early feature is cell swelling, not shrinkage. The chromatin aggregates peripherally, under the nuclear membrane, into dense masses of various shapes and sizes. The apoptotic cell first shows extensive surface membrane blebbing, which is followed by fragmentation of the dead cells into membranebound apoptotic bodies composed of cytoplasm and tightly packed organelles, with or without nuclear fragments.
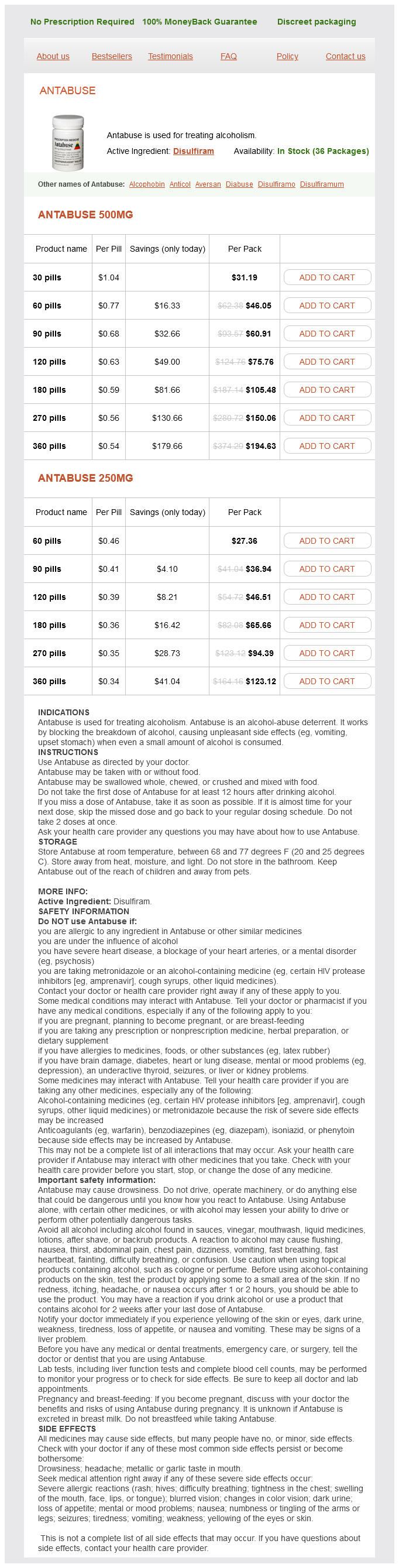
Antabuse Dosage and Price
Antabuse 500mg
- 30 pills - $31.19
- 60 pills - $46.05
- 90 pills - $60.91
- 120 pills - $75.76
- 180 pills - $105.48
- 270 pills - $150.06
- 360 pills - $194.63
Antabuse 250mg
- 60 pills - $27.36
- 90 pills - $36.94
- 120 pills - $46.51
- 180 pills - $65.66
- 270 pills - $94.39
- 360 pills - $123.12
Postinfectious cough is a diagnosis of exclusion in treatment 1-3 purchase antabuse paypal, and by definition it eventually resolves, but its duration may be prolonged. For this reason, 8 weeks is a more clinically useful working definition of chronic cough than 3 weeks. Vigorous coughing can stimulate esophageal reflux, which has been implicated as a cause of postinfectious cough. Active pertussis infection in adolescents and adults is an under-recognized cause of chronic cough. One investigation found a 21% incidence of pertussis in a group of patients with a cough duration of 2 weeks to 3 months. Patients experience periodic episodes of violent coughing, and post-tussive emesis is common. The inspiratory whooping sound typical in children is generally not heard in adults. Usually, cough begins within 1 week of starting the medication, but it can begin as late as 1 year later. Approximately 10% to 20% of patients develop cough, but in many it is not bothersome. Cancer Bronchogenic carcinoma is an infrequent cause of chronic cough (2%), although most patients with intrathoracic malignancies develop cough at some point in the course of their disease. Cough receptors are more highly concentrated in the larger airways; thus, cough is more common in malignancies with a predilection for central airways, such as squamous cell and small cell cancers. A history of tobacco use or new-onset cough or hemoptysis in a heavy cigarette smoker should heighten clinical suspicion. Prospective trials of chronic cough have found a 100% negative predictive value for a normal or unchanged chest x-ray, but the numbers in these studies were small. It is a diagnosis of exclusion and should not be entertained until all other potential causes have been investigated, with therapeutic trials of adequate intensity and duration. There are no distinguishing historical features to reliably differentiate it from other etiologies. In distinction, psychogenic cough usually implies an underlying psychiatric disorder. Most patients with psychogenic cough harbor an intractable fear of a serious underlying medical disease. Rare Causes of Chronic Cough Rare causes of chronic cough include interstitial lung disease. Disorders of any of the locations of cough receptors (external auditory canal, tracheobronchial tree, pleura, pericardium, diaphragm, esophagus, stomach) can also cause chronic cough. Patients who lack specific clues by history and examination and who have a normal chest x-ray and spirogram represent the most common management dilemma for the clinician. A major decision involves the extent of specific diagnostic testing as opposed to trials of empirical therapy. Randomized clinical trials do not provide adequate guidance to help the clinician choose between these two strategies. The approach is usually negotiated with the patient, partly based on the level of subjective distress and on the level of exasperation by the patient and the clinician. Features of cough, such as timing, associated sputum production, and cough character. Finally, there are no diagnostic tests with a sufficiently high positive predictive value to reliably implicate any particular cause of cough. A significant fraction of nonresponders fail treatment due to inadequate intensity or duration of treatment. One study found that the diagnosis was correct in 14% of referred patients, but the treatment regimens were insufficient. Common causes for diagnostic frustration include inadequate diagnosis and inadequate treatment. All tests used for evaluating chronic cough have a poor positive predictive value. Over-reliance on historical features or cough characteristics can thwart accurate diagnosis because these are often misleading. The cause of cough may be otherwise clinically silent, and 18% to 62% of chronic coughs are due to two or more causes. Diagnostic testing that suggests an underlying cause does not ensure that cough is caused by that etiology. Inadequate treatment regimens are a common reason for failure to alleviate symptoms, and eradication of related symptoms (heartburn, nasal congestion) does not ensure that an underlying cause is sufficiently treated. Central cough suppressants, such as dextromethorphan and codeine, should generally be avoided; they might serve as a temporizing measure but can distract from the search for a specific cause. The American College of Chest Physicians and the British Thoracic Society advise obtaining a chest x-ray before starting empirical therapy. Even with a finding of endobronchial pathology, the positive predictive value is only 50% to 89%. Occupational and environmental exposures should be considered as exacerbating factors in all patients who present with cough. Indoor allergens, such as pets and dust mites, and secondhand exposure to cigarette smoke are common environmental causes that are easily modifiable. Firstgeneration antihistamines, such as dexbrompheniramine maleate or azatadine maleate, have been demonstrated to be superior to second-generation (nonsedating) drugs, due to their additional anticholinergic activity. Second-generation antihistamines are useful primarily in allergic rhinitis syndromes. The role of bacteria in perpetuating chronic sinusitis is controversial, and treatment regimens are not well defined. Long-term use of topical decongestants should be discouraged to avoid rebound nasal congestion (rhinitis medicamentosa).