General Information about Amaryl
Amaryl has a good security profile and is usually well-tolerated, with the most common unwanted facet effects being delicate and transient, corresponding to nausea, headache, and dizziness. However, as with any medication, it could work together with other medication, so it is very important inform your physician of some other medicines you're taking earlier than starting Amaryl.
In addition to its blood sugar-lowering results, Amaryl has also been shown to produce other benefits in sufferers with type 2 diabetes. Studies have shown that it could possibly improve insulin sensitivity, which is a key issue within the improvement and development of diabetes. It has also been linked to reductions in fasting blood sugar levels, post-meal blood sugar spikes, and HbA1c levels, a measure of long-term glucose management. These advantages contribute to higher total glycemic control, which may help forestall long-term problems of diabetes corresponding to heart disease, kidney disease, nerve damage, and blindness.
Amaryl works by stimulating the pancreas to supply more insulin, thereby growing the physique's capability to control blood sugar ranges. This mechanism of action is shared by other sulfonylureas, making it a broadly used therapy choice for kind 2 diabetes. However, what units Amaryl other than other similar medicine is its long-acting nature. It has a half-life of about 5-8 hours and a duration of action of up to 24 hours, making it a handy once-daily medicine. This reduces the burden of multiple dosing and helps enhance treatment adherence, which is crucial for managing diabetes.
One of some great advantages of Amaryl over different sulfonylureas is its comparatively low danger of hypoglycemia, or dangerously low blood sugar levels. This is as a end result of of its potency and its capacity to stimulate insulin secretion in a glucose-dependent method. As a result, it's considered a safer possibility for elderly sufferers or these with kidney or liver problems, who're extra prone to hypoglycemia. However, it is very important observe that hypoglycemia can still occur if Amaryl just isn't taken in accordance with the prescribed dosage and proposals. Therefore, it is essential to comply with the directions of a healthcare professional while using this medicine.
Millions of individuals all over the world live with diabetes, a chronic illness that affects the body's ability to use or produce insulin, which is answerable for regulating blood sugar ranges. And with the rising prevalence of diabetes, there's a growing need for effective and accessible remedies. One such therapy is Amaryl, an oral blood sugar-lowering drug from the sulfonylurea class.
Amaryl, also recognized by its generic name glimepiride, has been used in the treatment of kind 2 diabetes since its approval by the united states Food and Drug Administration (FDA) in 1995. It is prescribed for sufferers who have not responded properly to lifestyle adjustments such as food plan and exercise, and who require additional help in controlling their blood sugar ranges.
In conclusion, Amaryl has been a extensively used and trusted therapy option for type 2 diabetes for over 20 years. Its long-acting nature, low risk of hypoglycemia, and useful effects on varied parameters of glycemic control make it a preferred selection for so much of healthcare professionals. However, it could be very important keep in thoughts that Amaryl just isn't a standalone therapy for diabetes, and it must be used in conjunction with way of life adjustments to attain optimum outcomes. If you've been prescribed Amaryl, it is necessary to observe your physician's instructions carefully and regularly monitor your blood sugar levels to make sure its effectiveness in managing your diabetes.
The history and physical examination could provide further leads and suggest additional focused laboratory testing for rare conditions (stool for ova, antitissue transglutaminase antibodies, lipase, gastrin, intestinal biopsy, or radiographic contrast studies for stasis, strictures, fistulas) diabetic diet how many carbs per day 2 mg amaryl order fast delivery. With no further leads, and therefore by default, one can assume that the diagnosis is either pernicious anemia or food-cobalamin malabsorption, which are both treated with similar replacement doses of cobalamin. Thus the history, physical findings, and focused laboratory tests with careful clinical follow-up can potentially identify the cause of the majority of cases of cobalamin deficiency and bypass the need for a Schilling test. Parenteral hydroxocobalamin should be reserved for all inborn errors of cobalamin metabolism. There is equivalence between oral 2-mg cobalamin tablets consumed daily (where cobalamin is passively absorbed at high doses) and traditional monthly parenteral treatment with 1 mg of intramuscular/ subcutaneous cobalamin among those requiring long-term cobalamin. So for patients who refuse monthly parenteral therapy, or prefer daily oral therapy, or in those with disorders of hemostasis, cobalamin (1 to 2 mg/day as tablets) can be recommended for all those patients with cobalamin malabsorption. However, if malabsorption of food-bound cobalamin is suspected (especially in the elderly with achlorhydria), higher doses of daily oral cobalamin (equal to or greater than 1000 mcg/day) is required. More than 98% of all the cobalamin in feces is in the form of cobalamin analogues, and about 80% of the ingested cobalamin is converted to analogues by microorganisms in the gut. If the underlying cause leading to folate deficiency is not corrected, folate may be continued. It is too expensive for conventional repletion in folate-deficient states in adults. Response to Replenishment the response of the patient to appropriate replacement is reversion of megaloblastic hematopoiesis to normal hematopoiesis within the first 12 hours; by 48 hours normal hematopoiesis is reestablished, and the only evidence for a prior megaloblastic state may be the persistence of a few giant metamyelocytes. Because megaloblastosis caused by cobalamin or folate deficiency can be reversed in 24 hours by administration of folate. Clinically the first 36 to 48 hours are often highlighted by the awakening of an occasional semistuporous individual whose "chief complaint" is amazement at the remarkably improved sense of well-being experienced, with increased alertness and appetite and reduced soreness of the tongue. This may precipitate an attack of gout if the patient has a "gouty predisposition. If pure folate deficiency has been prolonged, expect associated cobalamin deficiency to ensue (special emphasis should be given to identifying subtle manifestations of neurologic disease). An appropriate regimen for conditions in which cobalamin replenishment can correct cellular cobalamin deficiency (but not correct the underlying problem that led to the deficiency, such as pernicious anemia) is 1 mg of intramuscular or subcutaneous cyanocobalamin per day (week 1), 1 mg twice weekly (week 2), 1 mg/ week for 4 weeks, and then 1 mg per month for life (about 15%, or 150 mcg, is retained 48 hours after each 1-mg cobalamin injection). Ideally, this protocol for rapid correction of cobalamin deficiency and complete replenishment of cobalamin stores should be used in the beginning for all patients with cobalamin deficiency, regardless of the etiology (see box on Modified Therapeutic Trials). During this process, there may be a transient left shift to include myeloid precursors. In response to cobalamin, progression of neurologic damage and dysfunction is inhibited. In general the degree of functional recovery is inversely related to the extent of disease and duration of signs and symptoms. As a rough estimate, signs and symptoms that have been present for less than 3 months are usually completely reversible; with longer duration, there is invariable residual neurologic dysfunction. The reversibility of neurologic damage is slow (a maximal response may take 6 months). Substantial increments (in recovery) are unlikely to be gained after the first 12 months of appropriate therapy. However, most neurologic abnormalities have improved in up to 90% of patients with documented subacute combined degeneration. All women contemplating pregnancy (at least 400 mcg/day)§ Pregnancy and lactation, premature infants Mothers at risk for delivery of infants with neural tube defects ¶ Hemolytic anemias/hyperproliferative hematologic states Patients with rheumatoid arthritis or psoriasis on therapy with methotrexate# Patients on antiepileptic drugs Patients with ulcerative colitis *For vegetarians, prophylaxis with cobalamin (5- to 10-mcg tablet/day) orally should suffice. In all other conditions involving any abnormality of cobalamin absorption, cobalamin tablets of 1000 mcg/day should be administered orally to ensure that cobalamin transport by passive diffusion across the intestine is sufficient to meet daily needs. Consider late development of cobalamin deficiency and iron malabsorption (prophylaxis with oral cobalamin and iron). Ensure that the patient does not have a cobalamin deficiency before initiating long-term folate prophylaxis. Follow-Up Patients with neurologic dysfunction from cobalamin deficiency have traditionally been given more frequent doses of cobalamin (biweekly rather than monthly therapy for the first 6 months), despite the lack of evidence that this form of therapy is more beneficial. This approach nevertheless serves a purpose in that improvement in neurologic status can be carefully documented. Once maximal responses have been established, most patients can be treated with life-long cobalamin with a dose that is appropriate for the underlying cause of cobalamin deficiency. Follow-up outpatient visits every 6 months should be instituted to ensure adequate maintenance of hematopoiesis, as well as early diagnosis of other diseases commonly associated with the cobalamin- or folate-deficient state. Follow-up of patients with pernicious anemia suggest that individuals older than 60 years are prone to developing iron deficiency that arises from poor iron absorption from achlorhydria. Patients with pernicious anemia have a twofold increase in proximal femur and vertebral fractures and a threefold increase in distal forearm fractures. Finally, three studies (from Sweden, the United States, and Denmark) on a total of nearly 15,000 patients with pernicious anemia have identified an excess risk for gastric cancers within the first few years of diagnosis178; so it is prudent to recommend upper endoscopy for these patients. Food fortification with folic acid (140 mcg/100 g flour) has nearly eliminated folate deficiency179,180-the prevalence of low serum folate level decreased from 18. Supplementation with folate during pregnancy also helps to prevent premature delivery of low-birth-weight infants,8 and routine supplementation for premature infants and lactating mothers is also recommended. This program, which involved weekly ironfolic acid supplementation combined with a regular deworming program, was able to successfully improve the hemoglobin and iron status among 52,000 Vietnamese women of reproductive age. Anemia with a hemoglobin value of less than 11 g/dL is found in 75% of children191; although this is primarily related to low iron stores, there is also an association with low folate stores. There would be additional benefit of cobalamin supplements for women who are already at risk for cobalamin deficiency because of poverty-imposed near-vegetarianism or for those who are vegetarians. For schoolchildren, simple community-level interventions, such as micronutrient fortification (using a premix added to school lunch meals), that build upon the infrastructure of an existing program have proven to be contextually acceptable and efficacious in improving folate and cobalamin (in addition to vitamin A and iron) status in Himalayan villages of India.
In addition to myasthenia gravis, other paraneoplastic syndromes, such as acquiredhypogammaglobulinemia,pureredcellaplasia,Gravesdisease,pernicious anemia, dermatomyositis-polymyositis, and Cushing syndrome, can be seen blood glucose while fasting amaryl 2 mg low cost. It has a rapid onset, involves more widespread skin hardening, will generally cause much internal organ damage (especifically the lungs and gastrointestinal tract), and is generally more lifethreatening. The immune-cytochemical feature of Langerhans cell histiocytosis is positivity for which of the following A 70 years old male who has been chewing tobacco for the past 50 years presents with a six months history of a large, fungating, soft papillary lesions in the oral cavity. Two biopsies take from the lesion proper show benign appearing papillomatosis with hyperkeratosis and acanthosis infiltrating the subjacent tissues. Which of the following stains is used to detect lipid in frozen section biopsy in histopathology laboratory A 14 years old girl on exposure to cold develop pallor of extremities followed by pain and cyanosis. A patient presents with mediastinal mass with sheets of epithelial cells giving arborizing pattern of keratin reactivity along with interspersed lymphoid cells. Warthin-Finkeldey cells are seen in: (a) Measles (b) Rubella (c) Influenza (d) Rickettsial pox 31. Most common second malignancy in patients with familial retinoblastoma is: (Karnataka 2004) (a) Teratoma (b) Medullary carcinoma (c) Osteosarcoma (d) Malignant melanoma 35. Epulis is (a) Tumor of gingiva (b) Tumor of enamel of tooth (c) Disarrangementoftooth (d) Dysplasticleukoplakia 43. Triad of biotin deficiency is (a) Dermatitis,glossitis,steatorrhea (b) Dermatitis,glossitis,alopecia (c) Mental changes, diarrhea, alopecia (d) Dermatitis,dementia,diarrhea 45. Basophilic stippling is seen in: (a) Cadmium poisoning (b) Lead poisoning (c) Chromium poisoning (d) Iron poisoning 46. Pleomorphic adenoma usually arises from (a) Parotid gland (b) Submandibular gland (c) Minor salivary gland (d) Superficiallobe 48. Pellagra is characterized by all except: (a) Diarrhea (b) Dementia (c) Dermatitis (d) Diplopia 59. Smoking causes all cancers except: (a) Liver (b) Pancreas (d) Lung (c) Bladder 60. Prognostic factors in Neuroblastoma · Age and stage: Good prognosis in infants regardless of stage. Note: Most characteristic cytogenetic abnormality in neuroblastoma is 1p deletion. Features of verrucuous carcinomas · Predilection for males > 50 years · Predisposed in tobacco users, poor oral hygiene · Grossly, it is a soft, large, wart like (papillomatous) lesion which may show fungation · Microscopically: Cytological features of malignancy are absent or minimal and rare Epithelium is thickened and thrown into papillary folds the folds project both above and below the level of surrounding mucosa and crypt like surface grooves exhibit marked, pre-keratin plugging. Because some are too small to be detected cytogenetically, they are termed as microdeletion syndromes the important microdeletion syndromes are: 1. A pair of connexins from adjacent cells joins to form a gap junction that bridges the 2-4 mm gap between the cells. Thesuprabasal acantholytic blister that forms is characteristic of pemphigus vulgaris. The bullae are tense and oral lesions are present in 10-15% of affected individuals. The disease results from formation of antibodies against gliadin and is associated with celiac disease. Bydirectimmunofluorescence,dermatitisherpetiformis shows granular deposits of IgA selectively localized in the tips of dermal papillae. Itusuallyaffectsthe scalp, face, chest, and back, and the mucous membranes are only rarely affected. The blanching, or pallor, represents the ischemic phase of the phenomenon and results from vasospasm of digitalarteries. Occasionally, persistent digital ischemia develops and may result in ulcers or gangrene. In most severe cases, the small vessels are occluded by a proliferative endarteritis. Miscellaneous 662 Miscellaneous · Features of acrodermatitis enteropathica start appearing in the first few months of life, as the infant discontinues breastmilk. The skin lesions may be secondarily infected by bacteria such as Staphylococcusaureus or fungi like Candidaalbicans. Without treatment, the disease is fatal and affected individuals may die within a few years. Chief cells are neuroendocrine cells and are positive for regular neuroendocrine markers. It has been shown to increase in response to ventricular volume expansion and pressure overload. When somatic cells replicate a small section of the telomere is not duplicated and telomeres become progressively shortened. The loss of telomere function leads to activation of p53 dependent cell cycle checkpoints causing proliferative arrest or apoptosis. Germ cells, some stem cells and cancer cells continue to divide because in these cells telomere shortening is prevented · by sustained function of the enzyme telomerase that maintains the length of the telomere by nucleotide addition. Histologically one sees a proliferation of spindle cells andendothelialcells,extravasationofredbloodcells,hemosiderin-ladenmacrophages,and,inearlycases,aninflammatorycellinfiltrate. They are seen in the · Articular cartilage of joints* · Periarticular ligaments* · Tendons and soft tissues* · Achilles tendon* · Ear lobes* Other important points · Most common joint involved in Gout is Big Toe (First metatarsophalangeal joint) Miscellaneous 664 Miscellaneous · the diagnosis is made by presence of monosodium urate crystal in polarized light which are needle shaped and strongly negative birefringent crystal. In Niemann-Pick disease, they are widely distributed in spleen, liver, lymph nodes, bone marrow, and tonsils. Langhans giant cells Touton giant cells Tumour giant cells Foreign body giant cells Giant cells 1.
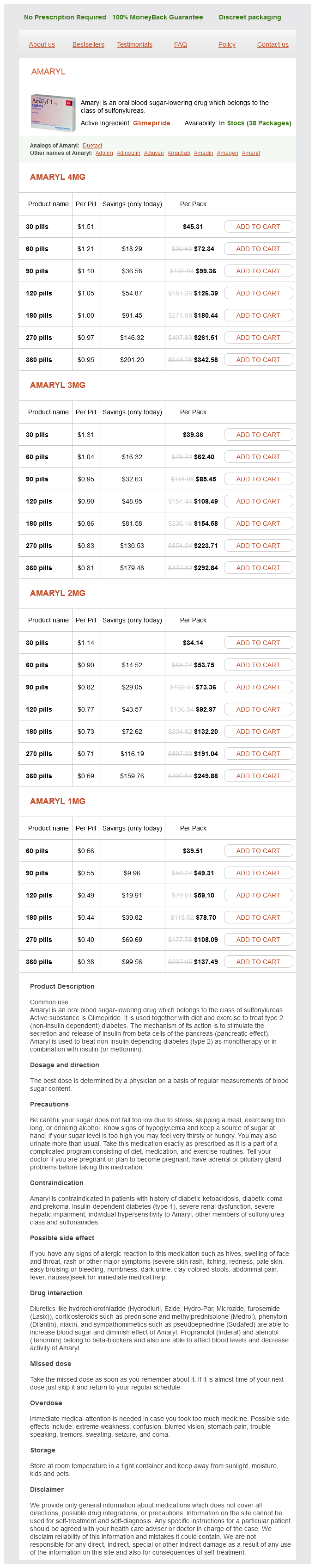
Amaryl Dosage and Price
Amaryl 4mg
- 30 pills - $45.31
- 60 pills - $72.34
- 90 pills - $99.36
- 120 pills - $126.39
- 180 pills - $180.44
- 270 pills - $261.51
- 360 pills - $342.58
Amaryl 3mg
- 30 pills - $39.36
- 60 pills - $62.40
- 90 pills - $85.45
- 120 pills - $108.49
- 180 pills - $154.58
- 270 pills - $223.71
- 360 pills - $292.84
Amaryl 2mg
- 30 pills - $34.14
- 60 pills - $53.75
- 90 pills - $73.36
- 120 pills - $92.97
- 180 pills - $132.20
- 270 pills - $191.04
- 360 pills - $249.88
Amaryl 1mg
- 60 pills - $39.51
- 90 pills - $49.31
- 120 pills - $59.10
- 180 pills - $78.70
- 270 pills - $108.09
- 360 pills - $137.49
Sorting Into Regulated Secretory Granules In regulated secretion, proteins are condensed into stored secretory granules that are released to the plasma membrane after the cell has received an appropriate stimulus blood sugar 01 amaryl 4 mg buy on line. Mature secretory granules are thought to be stored in association with microtubules until the stimulation of a surface receptor triggers their exocytosis. Conjugation of a cytotoxic T cell with its target causes its microtubules and associated secretory granules to reorient toward the target cell. Subsequently, the granules are delivered along microtubules until they fuse with the plasma membrane, releasing their contents for lysis of the Phagocytosis During phagocytosis cells are able to ingest large particles (greater than 0. Phagocytosis serves not only to engulf and destroy invading bacteria and fungi but also to clear cellular debris at wound sites and to dispose of aged erythrocytes. Primarily, specialized cells such as macrophages, neutrophils, and dendritic cells execute phagocytosis. Phagocytosis is triggered when specific receptors contact structural triggers on the particle, including bound antibodies, complement components as well as certain oligosaccharides. Then the polymerization of actin is stimulated, driving the extension of pseudopods, which surround the particle and engulf it in a vacuole called phagosome. The engulfed material is destroyed when the phagosome fuses with a lysosome, exposing the content to hydrolytic enzymes. Following invagination and budding, the vesicle becomes part of the endosome system, which is described in the following section. In some cells, pinocytosis can result in turnover of the entire plasma membrane in less than 1 hour. Receptor-Mediated Endocytosis this is a means to import macromolecules from the extracellular fluid. Some receptors are internalized continuously whereas others remain on the surface until a ligand is bound. In either case, the receptors slide laterally into coated pits that are indented regions of the plasma membrane surrounded by clathrin and pinch off to form clathrin-coated vesicles. The endosome is part of a complex network of interrelated membranous vesicles and tubules termed the endolysosomal system. It is still a matter of debate whether these structures represent independent stable compartments or whether one structure matures into the next. Lysosomes are also used for digestion of obsolete parts of the cell in the process of autophagy (described in more detail earlier). During the formation of clathrin-coated vesicles, clathrin molecules do not recognize cargo receptors directly but rather through the adaptor proteins, which form an inner coat. For receptors that are internalized in response to ligand binding, the internalization signal may also be generated by a conformational change induced by the binding of the ligand. These regulatory proteins also ensure that membrane traffic to and from an organelle are balanced. After budding, vesicles are transported to their final destination by diffusion or motor-mediated transport along the cytoskeletal network (microtubules or actin). The molecular motors kinesin, dynein, and myosin have been implicated in this process. The vesicles undergo an uncoating process before fusion with the correct target membrane. Both transport vesicles and target membranes display surface markers that selectively recognize each other. Protein motifs and their cognate receptors have been identified for many intracellular sorting and processing reactions. Studies are now directed to elucidate these processes at a molecular level by resolution of the three-dimensional structures of the proteins involved in protein processing and trafficking. The future challenge will be to find ways of exploiting this knowledge to intervene in the numerous disease states that result from errors in these processes. Brocker C, Engerlbrecht-Vandrè S, Ungermann C: Multisubunit tethering complexes and their role in membrane fusion. Kundu M, Lindsten T, Yang C, et al: Ulk1 plays a critical role in the autophagic clearance of mitochondria and ribosomes during reticulocyte maturation. Margittai E, Sitia R: Oxidative protein folding in the secretory pathway and redox signaling across compartments and cells. Schmidt O, Pfanner N, Meisinger C: Mirochondrial protein import: From proteomics to functional mechanisms. Tabas I, Ron D: Integrating the mechanisms of apoptosis induced by endoplasmic reticulum stress. In this chapter, we briefly outline the chemical structure of proteins and their posttranslational modifications. We explain how the properties of the 20 amino acids of which proteins are composed allow these polymers to fold into compact, functional domains and how particular domains and motifs have been assembled, modified, and reused in the course of evolution. Finally, we describe a sampling of proteins and domains of relevance to the hematologist and explore briefly how point mutations, chromosomal translocations, and other genetic alterations may modify protein structure and function to cause disease. All of the amino acids share a common core or backbone structure and differ only in the side chain emanating from the central -carbon of this core. The common backbone elements include an amino group, the central -carbon, and a carboxylic acid group. Peptide bonds are formed by reaction of the carboxylic acid of one amino acid with the amino group of the next amino acid in the chain. The resonant, partial double-bond character of the peptide bond prevents rotation about this bond; thus the five main-chain carbon, nitrogen, and oxygen atoms of each peptide unit lie in a plane. The conformational flexibility in the polypeptide chain is conferred by rotation about the bonds on either side of the -carbon atom; these bond angles are referred to as phi and psi angles.